Dental luxation and avulsion injuries in Hong Kong primary school children
Hong Kong Med J 2015 Aug;21(4):339–44 | Epub 17 Jul 2015
DOI: 10.12809/hkmj144433
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
ORIGINAL ARTICLE
Dental luxation and avulsion injuries in Hong Kong primary school children
SY Cho, MDS (Otago), FHKAM (Dental Surgery)
MacLehose Dental Centre, G/F, 286 Queen’s Road East, Wanchai, Hong Kong
Corresponding author: Dr SY Cho (rony_cho@dh.gov.hk)
 Full
paper in PDF
Full
paper in PDF
Abstract
Objectives: To identify the major causes and types
of dental luxation and avulsion injuries, and their
associated factors in primary school children in
Hong Kong.
Design: Case series.
Setting: School dental clinic, New Territories, Hong Kong.
Patients: The dental records of children with a
history of dental luxation and/or avulsion injury
between November 2005 and October 2012 were
reviewed. Objective clinical and radiographical
findings at the time of injury and at follow-up
examinations were recorded using a standardised
form. Data analysis was carried out using the Chi
squared test and multinomial logistic regression.
Results: A total of 220 children with 355 teeth of
dental luxation or avulsion injury were recorded.
Their age ranged from 6 to 14 years and the female-to-male ratio was 1:1.8. The peak occurrence was
at the age of 9 years. Subluxation was the most
common type of injury, followed by concussion.
Maxillary central incisors were the most commonly
affected teeth. The predominant cause was fall and
most injuries occurred at school. Incisor relationship
was registered in 199 cases: most of them were Class
I. Comparison of the incisor relationship in study
children and the general Chinese population in
another study revealed a higher proportion of Class II
and fewer Class III occlusions in the trauma group
(P<0.0001).
Conclusion: Most dental luxation and avulsion
injuries in Hong Kong primary school children are
caused by fall. Boys are more commonly affected
than girls, and a Class II incisor relationship is a
significant risk factor.
New knowledge added by this study
- This is the first epidemiological study of traumatic dental injury in children residing in Hong Kong. The present findings provide an important baseline for future comparison.
- As most injuries occur at school, it may be beneficial to educate primary school teachers about emergency care of children with dental trauma.
Introduction
Childhood injury is a major cause of death and
disability in many countries, including Hong
Kong.1 Although previous studies have reviewed
general childhood injuries in Hong Kong children,1 2 dental injuries have not been specifically studied
and reported. The oral region comprises 1% of the
total body area, yet a population-based study in
Sweden showed that it accounts for 5% of all body
injuries at all ages.3 A recent study conducted by
the Department of Health showed that injuries to
orofacial areas accounted for 1.7% of all body injuries
in children aged 14 years or below.1
Dental luxation and avulsion injuries account
for 15% to 61% of all dental traumas to permanent
teeth.4 It is an important public health concern as the
treatment of such injuries is often complicated and
requires specialist care.5 6 It also tends to occur at a young age during which growth and development
take place and so long-term follow-up is needed.5 6 7
The average number of dental visits because of
trauma to a permanent tooth during 1 year has been
shown to be much higher than that required for a
bodily injury.6 Information on how and where dental
trauma occurs, and the associated risk factors are
important data that can be used to plan a preventive
strategy. There is, however, little information about
the epidemiology of dental trauma in children
residing in Hong Kong. The aims of this retrospective
study were to identify the major causes and types
of dental luxation and avulsion injuries, and their
associated factors in primary school children
attending a school dental clinic in Hong Kong.
Methods
This retrospective study was carried out at Fanling
School Dental Clinic that provides care for
approximately 30 000 primary school children in the
Hong Kong New Territories East region. The study
materials comprised dental records of patients with
a history of dental luxation and/or avulsion injury
between November 2005 and October 2012. All
dental luxation and avulsion injuries were logged
in the electronic records using specific codes: an
electronic search of records was performed using
the same dental condition codes (DC=concussion,
DS=subluxation, DE=extrusion, DN=intrusion,
DL=lateral luxation, and DA=avulsion). All cases
were examined clinically by at least one of the three
attending paediatric dentists at the clinic who were
experienced in treating children with dental trauma.
All records were reviewed by one single examiner,
the paediatric dentist in-charge of the clinic.
Information was recorded in Microsoft Excel and
data analysis was carried out using the Chi squared
test and multinomial logistic regression with PASW
Statistics 18 software (SPSS Inc, Chicago [IL],
US). The level of significance was set at P<0.05.
To evaluate intra-examiner reliability, all selected
records were reviewed by the same author 1 month
after the original analysis and the findings of the two
examinations compared for discrepancies.
Clinical examinations
Since November 2005, a standardised dental trauma
form has been used in the clinic to facilitate follow-up
care. The following parameters
were recorded for patients who presented with
dental luxation or avulsion injuries: date and time
of injury, place where the injury occurred, cause
of trauma, presence of other orofacial soft tissue
injury, and the incisor relationship according to the
British Standard Incisor Classification.8 The type
of injury was classified according to the Andreasen
modification of the World Health Organization
classification,9 and included six types of injury to
periodontal tissues (Table 1).
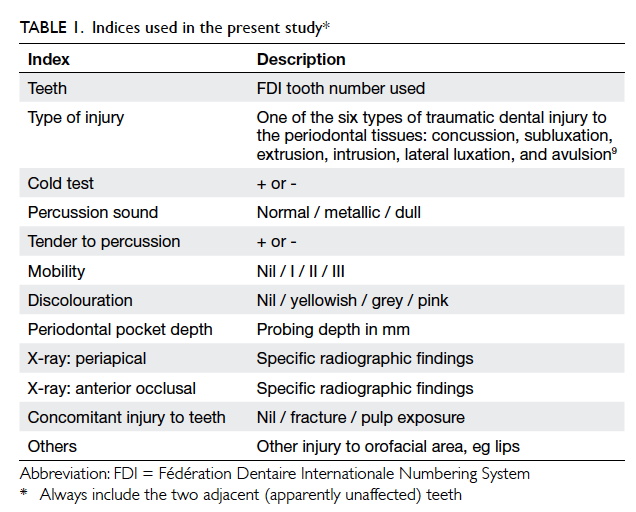
Table 1. Indices used in the present study
The adjacent apparently unaffected teeth on
both sides were also included in the examination.
For each tooth, objective clinical findings from the
initial and follow-up examinations were recorded
using the same standardised format and included
the following: pulp sensitivity test; percussion tone;
tenderness to percussion; tooth mobility; tooth
colour; periodontal probing depths; and the presence
of concomitant crown fractures and pulp exposure.
Radiographic examinations
An anterior occlusal radiograph together with
periapical radiographs of the affected teeth were
taken at the initial examination. At each follow-up
appointment, periapical radiographs were repeated
for the affected teeth. All periapical radiographs
were taken using a standard film holder (Dentsply
Rinn, Elgin [IL], US).
Follow-up examinations
All cases were followed up at regular intervals: 3
weeks, 6 to 8 weeks, 6 months, and then annually from
the time of injury. Patients with dental avulsion were
also seen on days 7 to 10 for splint removal and root
canal treatment if indicated.
Results
A total of 220 children with 355 teeth of dental
luxation or avulsion injury were recorded during the
study period. Their ages ranged from 6 to 14 years
(mean age, 9.2 years; standard deviation, 1.7 years). To
assess whether age was an important factor, children
were divided into two age-groups: 58% (n=128) were
aged 6 to 9 years and 42% (n=92) were 10 to 14 years at
the time of injury. The male-to-female ratio was 1.8:1,
with 141 boys and 79 girls. The gender difference in
prevalence was more prominent in children aged 9
years or above. The peak occurrence was seen at the
age of 9 years (n=46), followed by the age of 8 years
(n=44) and 10 years (n=38). Only one tooth was
traumatised in 117 (53%) children. The predominant
traumatic dental injury was subluxation, followed
by concussion (Table 2). Over 65% of teeth with
concussion or subluxation also had crown fractures.
Maxillary central incisors (295 teeth) were the most
commonly affected, followed by maxillary lateral
incisors (38 teeth) and mandibular incisors (20
teeth). The cause of injury was recorded in 219 cases
(Table 3). Fall (62%) was the predominant cause in
both genders and age-groups, followed by collision
(18%) and cycling (15%). There were no incidents of
injury caused by motor vehicle accidents or fights.
Statistical analysis using Chi squared test showed no
significant difference in the cause of injury between
genders (P=0.108) or between the two age-groups
(P=0.193). The place where the injury occurred
was recorded in 217 cases: most occurred at school
(Table 4). Statistical analysis using Chi squared
test showed a significant difference in the place of
occurrence between genders (Chi squared=15.6,
degrees of freedom=6, P<0.05), but no significant
difference between the two age-groups (P=0.078).
Multivariate analysis using multinomial logistic
regression was then performed with gender and age-group
as independent variables and place of injury
as a dependent variable. Because of the relatively
small number of cases, injuries that occurred in the
playground, street, swimming pool, and other places
were grouped into one category named as other
places in the analysis. Injury occurring at school
was then compared with injuries that occurred at
home, on a cycling path, or in other places. School
was chosen as the reference because (1) it was the
most common place where injury occurred; and
(2) univariate analysis of individual places of injury
using the Fisher’s exact test showed no significant
difference between genders regarding injuries
at school whereas there were significant gender
differences in injuries that occurred at home and on
a cycling path (P<0.05). The results of the regression
showed that boys were more commonly affected than
girls (P<0.05; odds ratio [OR]=2.97; 95% confidence
interval [CI], 1.05-8.43) for injuries that occurred
on a cycling path in comparison with injuries at
school. In the same model, younger children were
significantly less commonly affected than older
children (P<0.05; OR=0.42; 95% CI, 0.21-0.85)
for injuries that occurred in other places compared
with injuries at school.
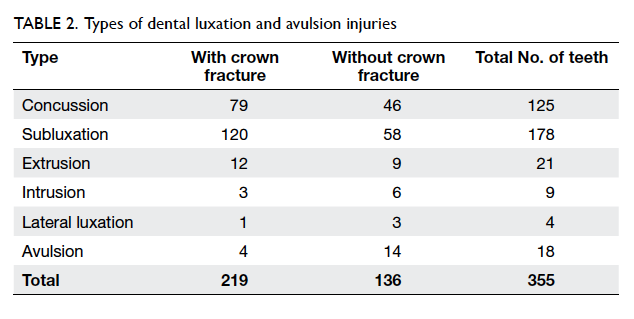
Table 2. Types of dental luxation and avulsion injuries
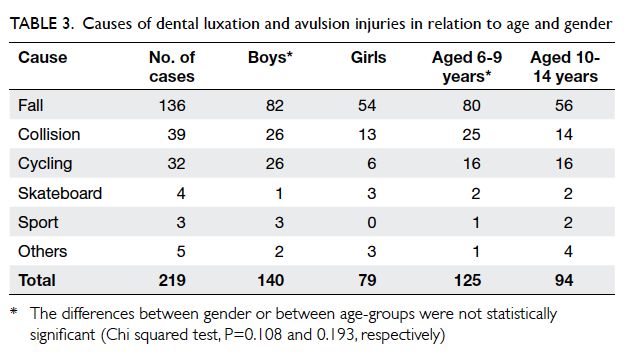
Table 3. Causes of dental luxation and avulsion injuries in relation to age and gender
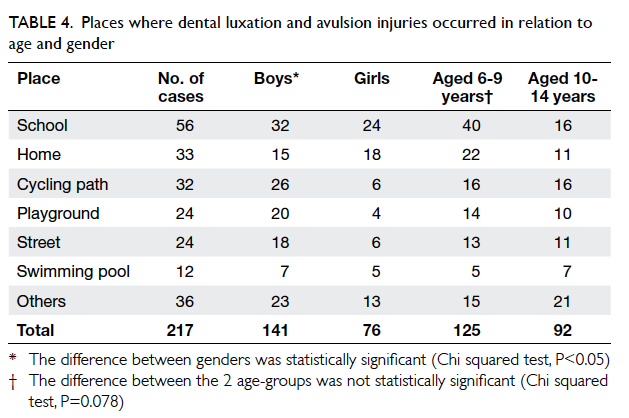
Table 4. Places where dental luxation and avulsion injuries occurred in relation to age and gender
Incisor relationship was registered in 199
cases: most were Class I (63%) [Table 5]. Since such
information was not available for the whole study,
it was decided to use data from a previous study
of the general Chinese population of children as a
retrospective comparison group.10 Comparison of
these two studies showed that there was a higher proportion of Class II and fewer Class III occlusions in
the trauma group than in the general Chinese
population. Statistical analysis showed a significant
difference between the two population groups (Chi
squared=36.1, degrees of freedom=2, P<0.0001).
Soft tissue injury occurred in the orofacial region in
87 children, and lips were involved in most instances
(82%). Intra-examiner reliability was evaluated and
complete concordance of all data and parameters
was found between the two evaluations that were 1
month apart.
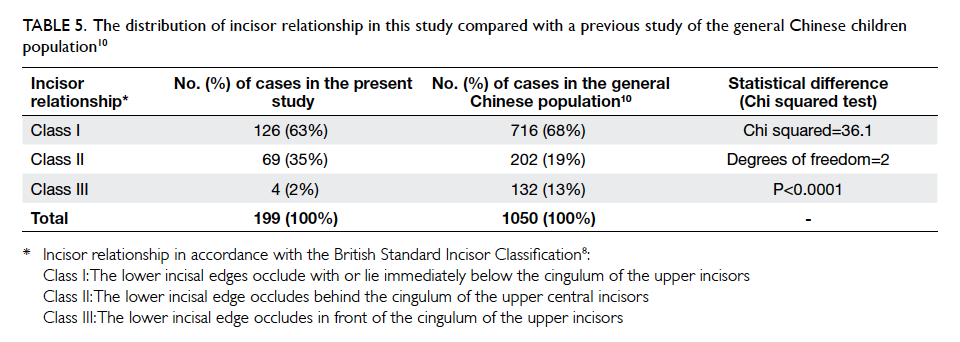
Table 5. The distribution of incisor relationship in this study compared with a previous study of the general Chinese children population10
Discussion
The difference in the proportion of causes of
traumatic dental injury depends on various factors
including culture, age-group, and population.11 12 In some developing countries, the most common
cause of dental injury in children is violence.9 In this
study, fall against a hard object such as the ground was the cause in over 60% of cases. This finding is
in agreement with most other studies of traumatic
dental injury in children.7 11 12 13 14 15 16 17 18 19 20 In a study of New
Zealand children, fall was the most common cause
in children aged 5 to 7 years, but collision became
more common in the 8- to 10-year-old group.21
Nonetheless, such a trend was not observed in this
study. Although dental injury due to cycling accidents
was not uncommon in this study, this finding may
be confounded by the fact that New Territories East
has one of the busiest cycling path networks in Hong
Kong.2 The use of helmets offers little protection
to the lower face and jaw.9 It has been suggested
that modification of the helmet design to cover the
lower face may be beneficial. There were few sports-related
injuries observed in this study. This may be
because high-risk contact sports, such as rugby and
ice hockey,5 are not very popular among Hong Kong
primary school children. Compulsory use of mouth
guards in those who participate in such activities
may also be a contributing factor. There was no case
of trauma due to a road traffic accident; this may
reflect the legal requirement in Hong Kong for all
passengers to wear a car seatbelt.
In this study more boys than girls had dental
luxation and avulsion injuries in accordance with
the findings of most other studies.7 13 14 15 16 17 18 19 22 23 24 One probable reason for the gender difference is that
boys take more risks and participate more in sports
activities. Nonetheless this gender difference has
narrowed in recent studies, possibly due to an
increased interest in sports among girls, especially
in western societies.5 11 21 In this study, a greater
gender discrepancy in frequency of dental injury
was observed in the older age-group, in accordance
with the findings of Kania et al’s study of elementary
school children in the US.24
Previous studies of dental trauma in children
have shown that most injuries occur between
the age of 6 and 12 years.7 16 17 18 The present study
population comprised primary school children
attending a regional school dental clinic. The age of
most primary school children in Hong Kong falls
within the range of 6 to 12 years, and so most of
the dental injuries for this group of children could
be registered in this study. The peak occurrence of
injury was seen in 9-year-olds, again in agreement
with previous studies where the highest frequency
of trauma to permanent dentition was observed in
9- to 10-year-olds.12 19 Nonetheless in studies from New Zealand21 and Iraq,14 the highest frequency of dental injury occurred in 5- to 7-year-olds. Glendor
et al9 observed a marked increase in the incidence
of dental injury in boys aged 8 to 10 years, with the
incidence rather stable in girls. The same trend was
also seen in this study. This may reflect the more
vigorous play characteristics of boys in this age-group
than girls.9
The majority of dental injuries involve the
anterior teeth, especially the maxillary central
incisors. The maxillary lateral and mandibular
incisors are affected less frequently.5 9 Similar findings were also observed in the present study. The
more prominent position of the maxillary central
incisors makes them more vulnerable to injury. In
addition, Kania et al24 opined that maxillary incisors
are more prone to injury than their mandibular
counterparts because of the mandible’s non-rigid
connection to the cranial base. Most of the children
in this study experienced trauma to only one tooth.
This concurs with the findings from previous
studies of dental injury in children.9 11 14 23 24 Noori and Al-Obaidi14 opined that when one tooth is
traumatised, the majority of the force is dispersed and so no more teeth will be injured.14 It has been suggested that multiple tooth injuries are seen
more often in more serious accidents such as motor
vehicle accidents and violence.8 9 24 Concussion and
subluxation together accounted for 85% of the cases
in this study, in accordance with the findings of most
previous studies on luxation and avulsion injuries
in children.7 16 17 19 21 As the force and direction of impact determines the resultant type of injury, the
findings from this study seem to suggest that most
periodontal tissue injuries in Hong Kong primary
school children are caused by more trivial incidents.9
Increased overjet and consequent incompetent lip
closure is a significant risk factor to traumatic dental
injury.7 9 13 14 15 22 23 24 In a study conducted in Iraq, 70%
of children who had a dental injury had increased
overjet.14 In many other studies, most children who
sustained a dental injury had normal overjet, yet the
percentage of children with increased overjet was
significantly higher in children with dental trauma
than in the general population.7 9
13 22 23 24 Similar
findings were also observed in the present study.
The more prominent tooth position and the lack
of a cushioning effect from the upper lip in Class
II malocclusion make the maxillary incisors more
prone to injury.14
In many previous studies, the predominant
place of injury occurrence in school-aged children
was home, followed by school and other public
places.9 13 21 22 In the present study, most injuries
occurred at school. The second and third most
common places of occurrence were home and cycling
paths, respectively. This finding was in agreement
with the population bodily injury survey of children
aged 14 years or below in Hong Kong.1 One probable
reason is that school children in Hong Kong have
relatively more play-time at school than at home. In
this study, 40% of children with a traumatic dental
injury also suffered soft tissue injury in the orofacial
region. This percentage was of similar magnitude
to another study that involved a large proportion of
children with dental luxation and avulsion injuries,17
but higher than a study with a high proportion of
minor dental trauma such as simple fracture.12 This
discrepancy may be because incidents that resulted
in dental luxation or avulsion were usually more
severe and could lead to more soft tissue damage.
One of the limitations of this study is its
retrospective design. It is, however, extremely
difficult to perform prospective trauma studies on a
population basis.25 ‘Grab’ sampling was employed in
this retrospective study, ie all patients treated in
one clinic for dental luxation and/or avulsion injury
were used in the sample. The conclusions from this
study may therefore not be applicable to other parts
of Hong Kong. To avoid inter-examiner error, all the
records were reviewed by the most senior paediatric
dentist in the clinic. The use of a standardised trauma
form helps improve the accuracy of data collected
during treatment.25 With the aid of a standardised
form, the cause of dental injury was recorded in all
but one case, and the place of trauma in all but three.
This illustrates the importance of a standardised
registry of dental traumatology.
This is the first epidemiological study of
traumatic dental injury in children resident in Hong
Kong and our data provide an important baseline
for future comparison. Very often, school teachers
are often the first to deal with an acute dental injury
and it may be beneficial to educate them about the
emergency care of children with dental trauma. For
example, with avulsion injuries, where immediate
management is critical for optimal healing, the
teachers should be taught how to replant the tooth
on site. If that could not be done, they should know
how to store the avulsed tooth in an appropriate
medium to prevent damage to the periodontal
tissue. The effects of various factors on healing will
be investigated and reported in a subsequent paper.
Dental traumas have social and economic
impacts with regard to the treatment required
but it is difficult to prevent dental injuries that are
not sports-related.6 21 One option is to improve environmental factors to prevent falling at school
and at home. Environmental and behavioural
factors, however, were not included in this study so
it is difficult to make conclusive suggestions in this
regard. Further studies are warranted.
Conclusion
The causes and types of dental luxation and avulsion
injuries in this group of Hong Kong children were
similar to those of other studies, except that more
injuries happened at school than at home. Most
dental luxation and avulsion injuries in Hong Kong
primary school children were caused by fall. Boys
were more commonly affected than girls, and Class
II incisor relationship was a significant risk factor.
Motor vehicle accident or fight was not a common
risk factor for dental injury in children. As most of
the injuries occurred at school, it may be beneficial
to educate primary school teachers about the
emergency care of children with dental trauma.
Acknowledgement
The author thanks Dr Denise Fung for her statistical
advice in this study.
References
1. Injury survey 2008. Hong Kong: Centre for Health
Protection, Department of Health; 2010.
2. Chan CC, Cheng JC, Wong TW, et al. An international
comparison of childhood injuries in Hong Kong. Inj Prev
2000;6:20-3. Crossref
3. Petersson EE, Andersson L, Sörensen S. Traumatic oral vs
non-oral injuries. Swed Dent J 1997;21:55-68.
4. Andreasen FM, Andreasen JO. Luxation injuries of
permanent teeth: general findings. In: Textbook and color
atlas of traumatic injuries to the teeth. 4th ed. Oxford:
Blackwell-Munksgaard; 2007; 372-403.
5. Glendor U. Epidemiology of traumatic dental injuries—a 12
year review of the literature. Dent Traumatol 2008;24:603-11. Crossref
6. Andersson L. Epidemiology of traumatic dental injuries.
Pediatr Dent 2013;35:102-5. Crossref
7. Zhang Y, Zhu Y, Su W, Zhou Z, Jin Y, Wang X. A
retrospective study of pediatric traumatic dental injuries in
Xi’an, China. Dent Traumatol 2014;30:211-5. Crossref
8. British standard incisor classification. Glossary of Dental
Terms BS 4492. London: British Standard Institute; 1983.
9. Glendor U, Marcenes W, Andreasen JO. Classification,
epidemiology and etiology. In: Textbook and color atlas of
traumatic injuries to the teeth. 4th ed. Oxford: Blackwell-Munksgaard; 2007: 217-54.
10. Lew KK, Foong WC, Loh E. Malocclusion prevalence in an
ethnic Chinese population. Aust Dent J 1993;38:442-9. Crossref
11. Andreasen JO, Bakland LK, Matras RC, Andreasen FM.
Traumatic intrusion of permanent teeth. Part 1. An
epidemiological study of 216 intruded permanent teeth.
Dent Traumatol 2006;22:83-9. Crossref
12. Eyuboglu O, Yilmaz Y, Zehir C, Sahin H. A 6-year
investigation into types of dental trauma treated in a
paediatric dentistry clinic in Eastern Anatolia region,
Turkey. Dent Traumatol 2009;25:110-4. Crossref
13. Bendo CB, Paiva SM, Oliveira AC, et al. Prevalence and
associated factors of traumatic dental injuries in Brazilian
schoolchildren. J Public Health Dent 2010;70:313-8. Crossref
14. Noori AJ, Al-Obaidi WA. Traumatic dental injuries among
primary school children in Sulaimani city, Iraq. Dent
Traumatol 2009;25:442-6. Crossref
15. Taiwo OO, Jalo HP. Dental injuries in 12-year-old Nigerian
students. Dent Traumatol 2011;27:230-4. Crossref
16. Sandalli N, Cildir S, Guler N. Clinical investigation of
traumatic injuries in Yeditepe University, Turkey during
the last 3 years. Dent Traumatol 2005;21:188-94. Crossref
17. Díaz JA, Bustos L, Brandt AC, Fernández BE. Dental
injuries among children and adolescents aged 1-15 years
attending to public hospital in Temuco, Chile. Dent
Traumatol 2010;26:254-61. Crossref
18. Toprak ME, Tuna EB, Seymen F, Gençay K. Traumatic
dental injuries in Turkish children, Istanbul. Dent
Traumatol 2014;30:280-4. Crossref
19. Atabek D, Alaçam A, Aydintuğ I, Konakoğlu G. A
retrospective study of traumatic dental injuries. Dent
Traumatol 2014;30:154-61. Crossref
20. Hecova H, Tzigkounakis V, Merglova V, Netolicky J. A
retrospective study of 889 injured permanent teeth. Dent
Traumatol 2010;26:466-75. Crossref
21. Chan YM, Williams S, Davidson LE, Drummond BK.
Orofacial and dental trauma of young children in Dunedin,
New Zealand. Dent Traumatol 2011;27:199-202. Crossref
22. Glendor U. Aetiology and risk factors related to traumatic
dental injuries—a review of the literature. Dent Traumatol
2009;25:19-31. Crossref
23. Zaragoza AA, Catalá M, Colmena ML, Valdemoro C.
Dental trauma in schoolchildren six to twelve years of age.
ASDC J Dent Child 1998;65:492-4,439.
24. Kania MJ, Keeling SD, McGorray SP, Wheeler TT, King GJ.
Risk factors associated with incisor injury in elementary
school children. Angle Orthod 1996;66:423-32.
25. Andersson L, Andreasen JO. Important considerations
for designing and reporting epidemiologic and clinical
studies in dental traumatology. Dent Traumatol
2011;27:269-74. Crossref