DOI: 10.12809/hkmj154626
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
LETTER TO THE EDITOR
MERS = SARS?
KL Hon, MD, FCCM
Department of Paediatrics, The Chinese University of Hong Kong, Prince
of Wales Hospital, Shatin, Hong Kong
Corresponding author: Prof KL Hon (ehon@cuhk.edu.hk)
 Full
paper in PDF
Full
paper in PDF
To the Editor—In 2003, the World Health
Organization coined the word “SARS” for severe
acute respiratory syndrome in patients with a
relevant travel/contact history and severe acute
respiratory symptoms.1 2 3 In 2012, the definition
of SARS was not used when monitoring another
outbreak of illness with the same symptoms and
viral aetiology.3 4 5 Instead, the virus was termed the
Middle East respiratory syndrome coronavirus
(MERS-CoV) and “MERS” has since become the
official nomenclature for the epidemic.3 In May
2015, a South Korean man travelled to Huizhou after
first arriving in Hong Kong. His father had recently
returned from Bahrain and was confirmed to have
been infected with MERS. The case aroused panic
about an outbreak of MERS beyond the Middle East
in Korea, and possible outbreaks in Hong Kong and
Mainland China. Meanwhile, the Hong Kong media
colloquially referred to the MERS outbreak as the
“new SARS”, despite the new official nomenclature.
MERS = SARS?
MERS and SARS are the same syndrome in that
both are caused by coronavirus, and are associated
with fever, respiratory symptoms, and a relevant
travel history (Table).5 In other words, the severity,
acuteness, and respiratory syndrome in MERS is no
less severe than SARS. There is no need to create a
new name and abbreviation each time a coronavirus
emerges.
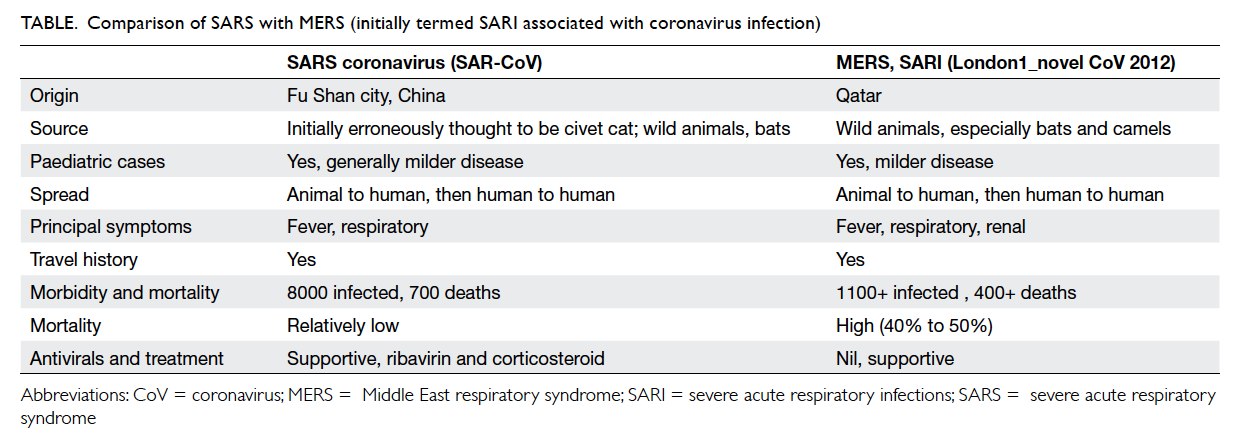
Table. Comparison of SARS with MERS (initially termed SARI associated with coronavirus infection)
MERS ≠ SARS?
Some experts opine that MERS carries a higher
mortality, and there is a travel or contact history
linked with the Middle East.4 In 2012, the initial
patients with MERS had non-respiratory (renal)
involvement and the MERS-CoV differed to the
SARS-CoV. On this basis, MERS and SARS are not
the same.
Health organisations should provide consistent
definitions for index surveillance and epidemiological
and prognostication studies. They should
resist the temptation to introduce unnecessary new
terminology each time an outbreak of the same
severe respiratory infection occurs.2 Diagnosis of
emerging infections should be laboratory-based and
not clinical or ‘syndrome’-based.
References
1. Hon KL, Leung CW, Cheng WT, et al. Clinical presentations
and outcome of severe acute respiratory syndrome in
children. Lancet 2003;361:1701-3. Crossref
2. Hon KL, Li AM, Cheng FW, Leung TF, Ng PC. Personal
view of SARS: confusing definition, confusing diagnoses.
Lancet 2003;361:1984-5. Crossref
3. Hui DS, Memish ZA, Zumla A. Severe acute respiratory
syndrome vs. the Middle East respiratory syndrome. Curr
Opin Pulm Med 2014;20:233-41. Crossref
4. Zumla A, Hui DS, Perlman S. Middle East respiratory
syndrome. Lancet 2015 Jun 3. Epub ahead of print. Crossref
5. Hon KL. Severe respiratory syndromes: travel history
matters. Travel Med Infect Dis 2013;11:285-7. Crossref