© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
REMINISCENCE: ARTEFACTS FROM THE HKMMS
The Schimmelbusch mask
Ronald Lo, FHKAM (Anaesthesiology), FRCA (Hon)
Guest author, Education and Research Committee, Hong Kong Museum of Medical Sciences Society
 Full
paper in PDF
Full
paper in PDF
Among the collection of the Hong Kong Museum of
Medical Sciences is a piece of equipment that was
used by anaesthetists all over the world from the end
of the 19th century until around the 1960s. Indeed,
it is still used in some resource-poor developing
countries after becoming obsolete in the developed
world; its use being dependent on the available
anaesthetic facilities. This is the Schimmelbusch
mask (Fig).
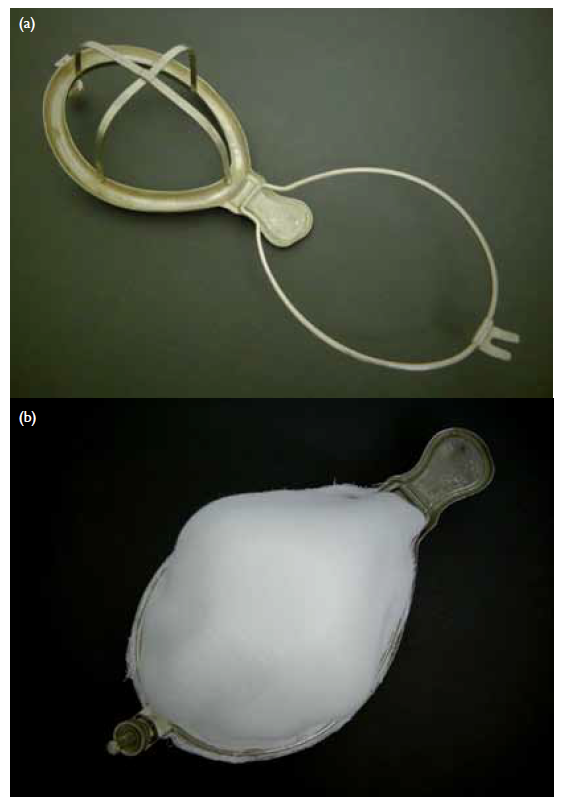
Figure. The Schimmelbusch mask, donated by the Department of Anaesthesiology, Queen Mary Hospital, to the Hong Kong Museum of Medical Sciences in March 1988. (a) It consists of a metallic oval frame with a gutter-like rim surmounted by crossing supports on which rests the Gamgee gauze with the anaesthetic agent, held in place by snapping down of the hinged metallic clamp as shown in (b). The desired amount of anaesthetic agent is dropped onto the gauze and the rim is used to prevent any excessive fluids from spilling onto the face of the patient
This mask was originally designed by Dr Curt
Theodor Schimmelbusch (1860-1895) in 1890 to
administer ether (or chloroform) to anaesthetise
patients undergoing surgery. Schimmelbusch
was also prominent in his day for studying steam
sterilisation and disinfection in surgery. It is a pity
he died relatively young at the age of 35 years from
tuberculosis. He graduated in medicine in 1886
from the University of Halle (now Martin-Luther
Universität Halle-Wittenberg) in Germany. He
worked in Halle (on steam sterilisation and wound
antisepsis) and Cologne but moved to Berlin soon
after. He introduced his anaesthetic mask while
working in Berlin, Germany.
Schimmelbusch attempted to improve his
original anaesthetic mask design in 1895 but it
was not a success; so the original design was used
in clinical practice. It has since been modified in
different ways but the principle remains the same.
The mask rim is designed to fit the contours of a
person’s face. A frame is constructed over the rim
of the mask with 10 to 12 layers of Gamgee gauze
(a surgical dressing invented by Dr Joseph Sampson
Gamgee in Birmingham, England, in 1880, consisting
of a thick layer of absorbent cotton wool held
between two layers of absorbent gauze) applied over
it and clamped in place during use. This frame keeps
the gauze away from the face of the patient to make
it more comfortable and acceptable for the patient.
There is a gutter that runs around the rim to catch
excess anaesthetic liquid so that it does not drip onto
the patient’s face and irritate the patient—this is a
desirable characteristic as an irritable patient might
contribute to stormy induction of ether anaesthesia.
When used, the mask with Gamgee gauze in
place is applied to the face of the patient. It covers
the nose and mouth while the liquid anaesthetic
(either chloroform or ether) is dropped onto the
gauze. The patient, thus, breathes through the gauze
and inhales the vapours of the anaesthetic. The
control of the anaesthetic dose and speed of onset
of effect are dictated by the anaesthetist controlling
the amount and rate of the liquid anaesthetic being
dropped onto the gauze. Ongoing anaesthesia
is maintained at the desired level by continued
administration of the liquid anaesthetic onto the
gauze, as appropriate.
The mask is classified as a semi-open
anaesthetic breathing system (circuit). As the mask
increases the anatomical dead space for breathing,
it causes an increase in the patient’s minute volume
ventilation in an attempt to compensate for the
reduction in alveolar ventilation. This physiological
ventilatory enhancement hastens the vaporisation
and inhalation of the anaesthetic and is conducive to
a quicker and less stormy induction.
The Schimmelbusch mask was probably used
in Hong Kong soon after its introduction to clinical
anaesthesia in the western world. As ether and
chloroform anaesthesia were prevalent in Hong Kong
from the early colonial days, with the first recorded
surgical operation performed on 18 March 1848 by
a British surgeon employing chloroform anaesthesia,
it is conceivable that the mask was generally used for
the purpose in Hong Kong since its invention and
introduction. Ether and chloroform were superseded
by the introduction of barbiturates (pentobarbital
and methohexital) for intravenous induction of
general anaesthesia and the use of inhalation
anaesthetic agents like trichloroethylene, and then
halothane, for induction or maintenance of general
anaesthesia in the 1950s. The mask was superseded
when new anaesthetic machines and breathing
circuits were designed after the Second World
War to vapourise and deliver volatile anaesthetics,
eg the Epstein-Macintosh-Oxford (EMO) ether
anaesthetic apparatus (1956), and the Boyle’s series
of Anaesthetic Machines (1950s to 1990s)—a British
anaesthetic equipment often used in Hong Kong at
the time. The EMO remained a back-up for the more
modern anaesthetic equipment (and for anaesthetic
training) in Hong Kong until the 1970s when they
were completely retired from service.