Hong Kong Med J 2014 Aug;20(4):351.e1–2
DOI: 10.12809/hkmj134057
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
PICTORIAL MEDICINE
Urinary bladder inguinal hernia: an uncommon
cause of scrotal swelling
HL She, MB, BS; KC Lam, MB, BS; KK Wong, MB, BS; Wendy WM Lam, MB, BS
Department of Radiology, Queen Mary Hospital, Pokfulam, Hong Kong
Corresponding author: Dr HL She (helenshe1025@gmail.com)
 Full
paper in PDF
Full
paper in PDF
A 77-year-old man with benign prostate hypertrophy
(BPH) presented to our hospital in October 2011
with a history of right groin swelling for several
months. He was otherwise asymptomatic. Physical
examination revealed a reducible right inguinal
hernia. Ultrasound (USG) examination of the groins
showed a fluid-filled lesion within the right scrotum.
It had a beaked appearance at its cranial portion,
which could be traced entering the right inguinal
canal (Fig 1a). A tiny calcified focus was noted within
this fluid-filled structure (Fig 1b). The normal right testis was displaced inferiorly (Fig 1c). Findings were
suggestive of urinary bladder inguinal hernia with
a bladder stone within. It was confirmed with non-contrast
computed tomography (CT) of the abdomen
and pelvis, which showed herniation of the urinary
bladder along the inguinal canal and into the right
scrotum, with a small bladder stone within (Fig 2).
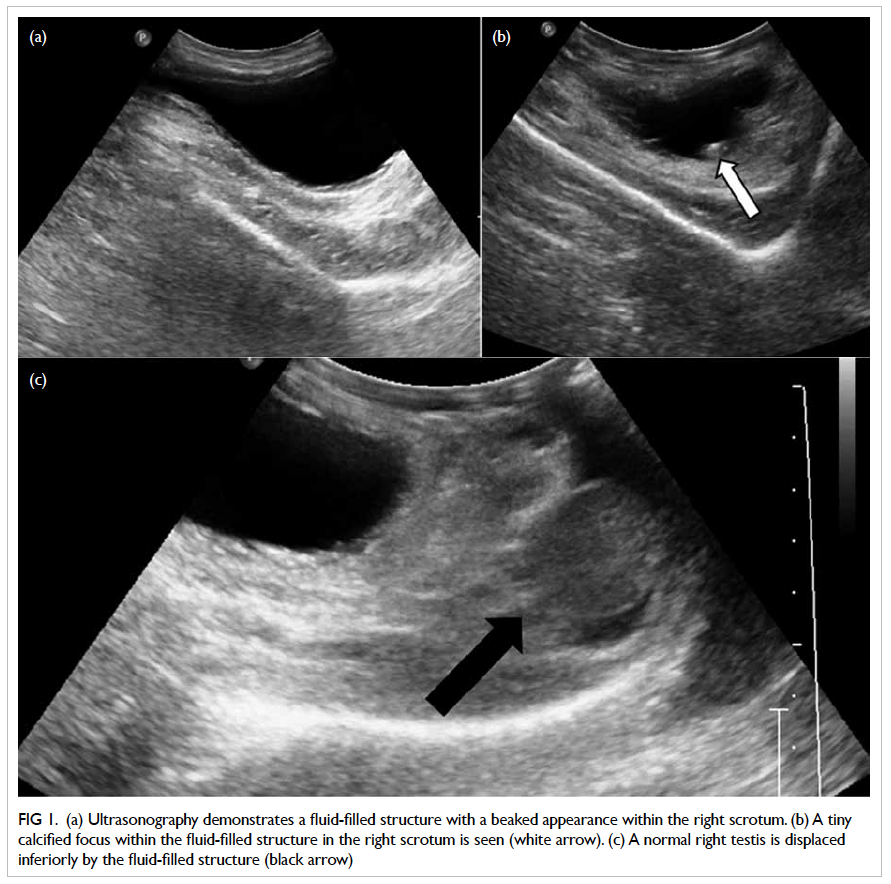
Figure 1. (a) Ultrasonography demonstrates a fluid-filled structure with a beaked appearance within the right scrotum. (b) A tiny calcified focus within the fluid-filled structure in the right scrotum is seen (white arrow). (c) A normal right testis is displaced inferiorly by the fluid-filled structure (black arrow)
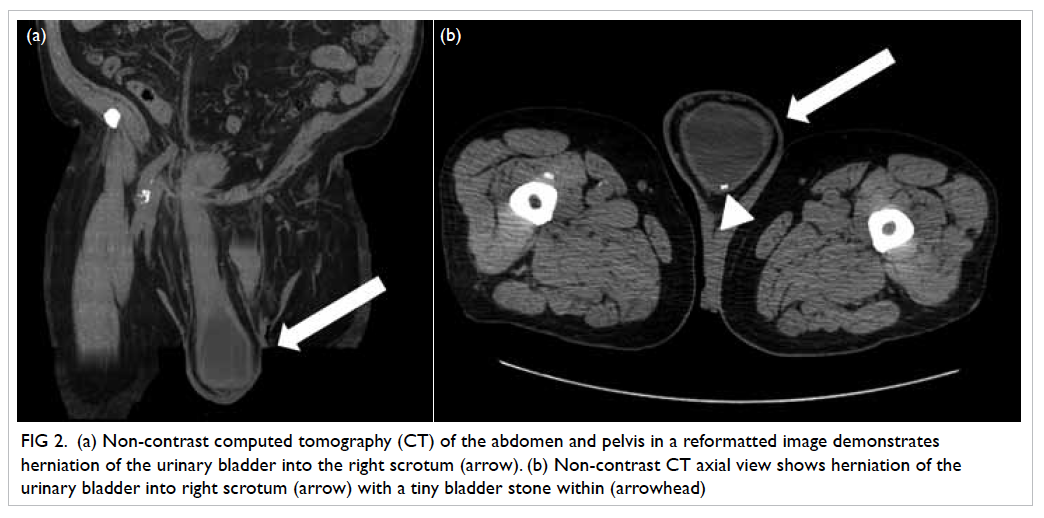
Figure 2. (a) Non-contrast computed tomography (CT) of the abdomen and pelvis in a reformatted image demonstrates herniation of the urinary bladder into the right scrotum (arrow). (b) Non-contrast CT axial view shows herniation of the urinary bladder into right scrotum (arrow) with a tiny bladder stone within (arrowhead)
Urinary bladder herniation is an uncommon
condition, encountered in 1% to 4% of inguinal
hernias. However, over the age of 50 years, the
frequency increases to about 10%.1 Most patients are asymptomatic and usually found incidentally on
imaging for workup of inguinal hernias, or even at
the time of herniorrhaphy. Occasionally, patients
may complain of urinary symptoms especially at
an advanced stage, and may entail double-phase
urination, that is, manually compressing the scrotum
for complete bladder emptying. Predisposing factors
include obesity, bladder outlet obstruction (eg due
to BPH), and weakened abdominal musculature.2
Imaging modalities including USG, intravenous
urogram, CT, and magnetic resonance imaging
usually facilitate the diagnosis. Standard treatment
entails surgical repair. It is important to be aware
of this diagnosis, as apart from complications
like urinary tract obstruction, urinary traction
infection and urinary bladder infarction, unknowing
herniorrhaphy may lead to bladder injury.1 3
References
1. Bisharat M, O’Donnell ME, Thompson T, et al.
Complications of inguinoscrotal bladder hernias: a case
series. Hernia 2009;13:81-4. CrossRef
2. Vindlacheruvu RR, Zayyan K, Burgess NA, Wharton SB,
Dunn DC. Extensive bladder infarction in a strangulated
inguinal hernia. Br J Urol 1996;77:926-7. CrossRef
3. Oruç MT, Akbulut Z, Ozozan O, Coşkun F. Urological
findings in inguinal hernias: a case report and review of
the literature. Hernia 2004;8:76-9. CrossRef