Hong Kong Med J 2024;30:Epub 22 Aug 2024
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
CASE REPORT
Aggressive renal angiomyolipoma with renal vein and inferior vena cava thrombus: a case report
Phoebe HW Lo, MB, BS1; HM Kwok, MB, BS, FRCR1; FH Ng, MB, ChB, FRCR1; HY Lo, MB, BS, FHKAM (Pathology)2; Johnny KF Ma, MB, BS, FRCR1
1 Department of Radiology, Princess Margaret Hospital, Hong Kong SAR, China
2 Department of Pathology, Princess Margaret Hospital, Hong Kong SAR, China
Corresponding author: Dr Phoebe HW Lo (lph218@ha.org.hk)
 Full paper in PDF
Full paper in PDF
Case presentation
A 58-year-old Chinese woman with good past
health presented with a 2-day history of right lower
abdominal pain. Routine biochemical blood tests
revealed a white blood cell count of 9.1 × 109/L and
normal renal function (creatinine level: 49 μmol/L).
An urgent contrast-enhanced computed tomography
scan revealed acute diverticulitis in the caecum.
Incidentally, a solitary well-defined homogenous
fat-density mass with unenhanced density of -63
Hounsfield units was evident at the right renal sinus,
with extension into the right renal vein and inferior
vena cava (IVC) [Fig 1]. Findings were suggestive of
an aggressive renal angiomyolipoma (AML) with
right renal vein and IVC thrombus. The patient
was referred to an urologist. Subsequent robotic-assisted
laparoscopic radical nephrectomy and IVC
thrombectomy were performed uneventfully.
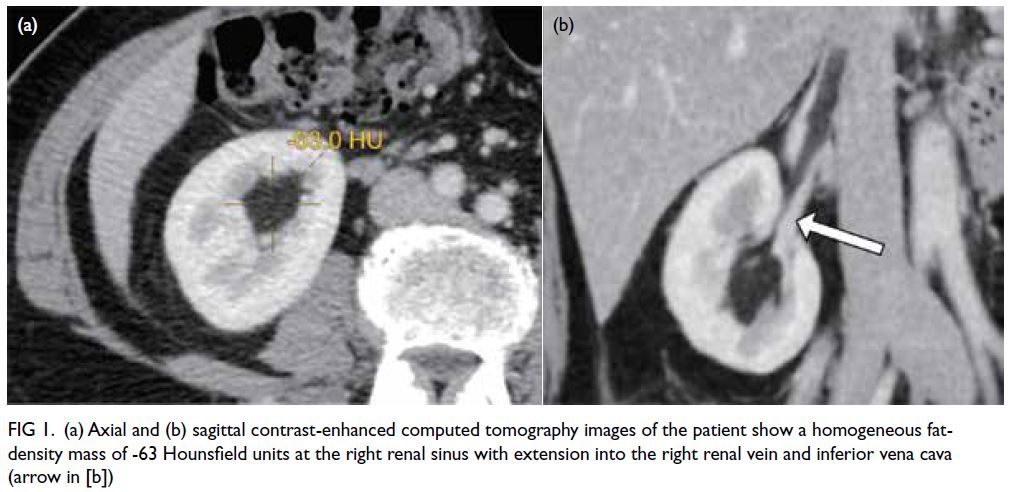
Figure 1. (a) Axial and (b) sagittal contrast-enhanced computed tomography images of the patient show a homogeneous fat-density mass of -63 Hounsfield units at the right renal sinus with extension into the right renal vein and inferior vena cava (arrow in [b])
The surgical specimen provided by the pathologist demonstrated the right renal vein depicted as a purple red strip and fatty tumour (Fig 2a). Microscopic examination revealed all features of a typical AML including mature adipocytes, myoid spindle cells, and thick-walled blood vessels (Fig 2b).
It was also positive on Melan A (Fig 2c) and HMB-45
stains (Fig 2d).
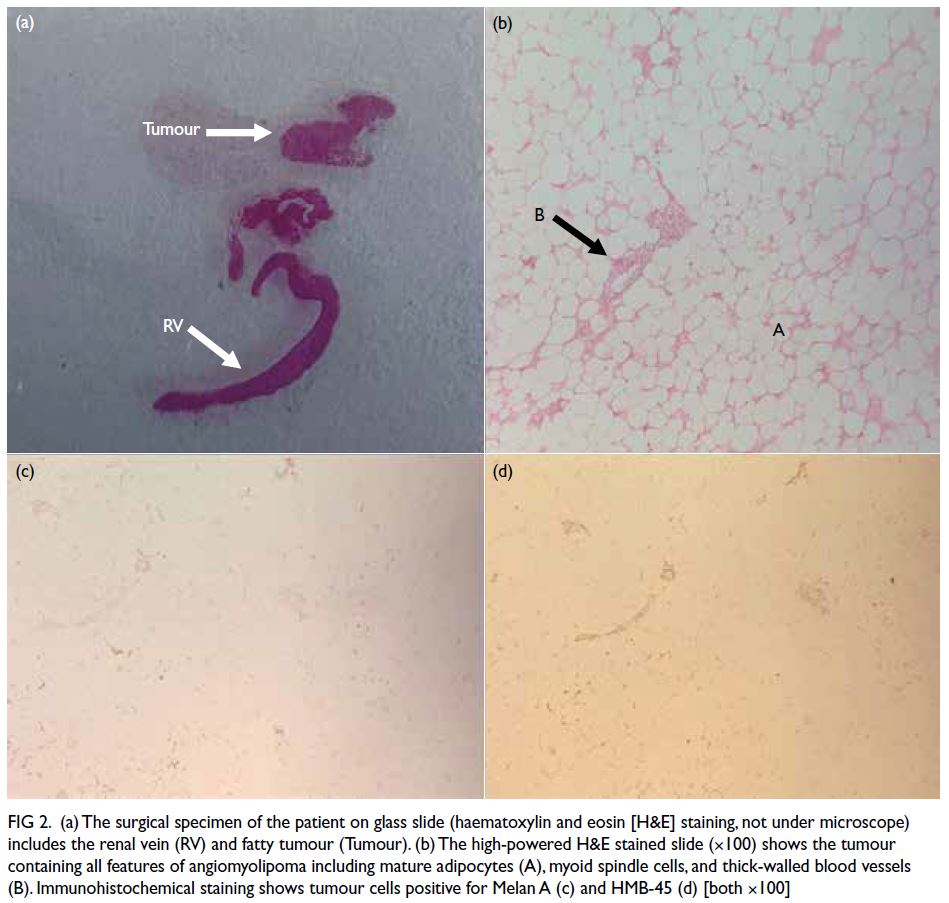
Figure 2. (a) The surgical specimen of the patient on glass slide (haematoxylin and eosin [H&E] staining, not under microscope) includes the renal vein (RV) and fatty tumour (Tumour). (b) The high-powered H&E stained slide (×100) shows the tumour containing all features of angiomyolipoma including mature adipocytes (A), myoid spindle cells, and thick-walled blood vessels (B). Immunohistochemical staining shows tumour cells positive for Melan A (c) and HMB-45 (d) [both ×100]
Discussion
Angiomyolipoma is a common benign renal
mesenchymal neoplasm composed in variable
proportions of adipose tissue, smooth muscle cells,
and abnormal vessels. It is most commonly sporadic
(80%) or associated with genetic syndromes such as
tuberous sclerosis.1 A renal mass with visualisation of
macroscopic fat density on computed tomography is
virtually diagnostic of AML. Therefore, visualisation
of fat density in the intravascular compartment is
indicative of tumour invasion.
Cases of aggressive AML with renal vein and
IVC thrombus have been reported. A literature
review2 of 26 cases of invasive renal AML reported
that a large size and right-sided location of the
tumour may be contributing factors in AML with
intravascular invasion. This may be related to the
shorter and straighter course of the right renal vein.
Two variants of renal AML, namely, classic and epithelioid, have been described. The epithelioid
variant has been reported to exhibit aggressive
behaviour with IVC thrombus.3 In this case, the
patient had a classic subtype of renal AML with
mature adipocytes (Fig 2b) and no epithelioid cells.
The optimal treatment is robotic nephrectomy
and IVC thrombectomy irrespective of tumour size,
since IVC thrombus can be life threatening with
higher risks of vessel occlusion and tumour embolus.
A multi-institutional study in 2016 retrospectively
reviewed 32 cases of robotic radical nephrectomy and
IVC thrombectomy and demonstrated a favourable
outcome with adequate robotic experience including
less blood loss, earlier patient discharge, and fewer
complications compared with open nephrectomy.4
Inferior vena cava thrombectomy follows similar
surgical principles to that for renal cell carcinoma
with IVC thrombus. Proper visualisation and
mobilisation of the kidney, renal vein and IVC allow selective vascular clamping, namely, the infrarenal
and suprarenal IVC as well as the renal vein. The
IVC is then exposed and the tumour is dissected
away from the IVC. The cavotomy is then closed and
nephrectomy is performed.
We describe a classic subtype of renal AML
extending into the renal vein and IVC, managed
by robotic-assisted laparoscopic nephrectomy and
IVC thrombectomy. Computed tomography and
other imaging modalities are essential to diagnose
AML and for proper surgical planning. With proper
visualisation of the kidney, renal vein and IVC, a safe
and successful outcome of robotic nephrectomy and
IVC thrombectomy is achieved.
Author contributions
Concept or design: PHW Lo, HM Kwok, FH Ng, JKF Ma.
Acquisition of data: PHW Lo, HM Kwok, FH Ng, HY Lo.
Analysis or interpretation of data: PHW Lo, HM Kwok, HY Lo.
Drafting of the manuscript: All authors.
Critical revision of the manuscript for important intellectual content: All authors.
Acquisition of data: PHW Lo, HM Kwok, FH Ng, HY Lo.
Analysis or interpretation of data: PHW Lo, HM Kwok, HY Lo.
Drafting of the manuscript: All authors.
Critical revision of the manuscript for important intellectual content: All authors.
All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Conflicts of interest
All authors have disclosed no conflicts of interest.
Funding/support
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
This study was approved by the Kowloon West Cluster Research Ethics Committee of Hospital Authority, Hong Kong [Ref No.: KW/EX-23-010(180-06)]. The patient has
given a consent statement for publication of this case report.
References
1. Martignoni G, Amin M.B. Pathology and genetics of
tumours of the urinary system and male genital organs.
In: Ebie JN, Sauter G, Epstein JI, editors. World Health
Organization Classification of Tumours. Lyon, France:
IARC; 2004: 65-7.
2. Islam AH, Ehara T, Kato H, Hayama M, Kashiwabara T,
Nishizawa O. Angiomyolipoma of kidney involving the
inferior vena cava. Int J Urol 2004;11:897-902. Crossref
3. Fox C, Salami SS, Moreira DM, et al. Aggressive renal
angiomyolipoma of the lipomatous variant with inferior
vena cava thrombus: a case report and review of the
literature. Urol Case Rep 2013;2:9-11. Crossref
4. Abaza R, Shabsigh A, Castle E, et al. Multi-institutional
experience with robotic nephrectomy with inferior vena
cava tumor thrombectomy. J Urol 2016;195:865-71. Crossref