Hong Kong Med J 2014;20:16–23 | Number 1, February 2014 | Epub 11 Sep 2013
DOI: 10.12809/hkmj133931
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
ORIGINAL ARTICLE
Physiotherapist-designed aquatic exercise
programme for community-dwelling elders with osteoarthritis of the
knee: a Hong Kong pilot study
Mary CK Lau, MHM, Prof Dip Phty;
Joseph KS Lam, Prof Dip Phty;
Eva Siu, MPH, Prof Dip Phty;
Carmen SW Fung, MScHC(PT), Prof Dip Phty;
Kevin TY Li, MHE&HP, Prof Dip Phty;
Margaret WF Lam, Prof Dip Phty
Shatin VHT Office, Elderly Health Service,
Department of Health, Room 326, Shatin Government Offices, 1
Sheung Wo Che Road, Shatin, Hong Kong
Corresponding author: Dr MCK Lau (mary_lau@dh.gov.hk)

Abstract
Objectives: To examine
the effectiveness and feasibility of a community-based
aquatic exercise programme for elders with osteoarthritis
of the knee.
Design: Prospective
intervention study, with a before-and-after design.
Setting: Community
elders.
Participants: Twenty
elders aged 65 years or above (mean, 72 years) attending
four Elderly Health Centres of the Department of Health who
had suffered from osteoarthritis of the knee for at least 3
years
and with mild-to-severe knee pain.
Intervention: A 10-week
aquatic exercise programme designed and led by
physiotherapists.
Main outcome measures: Range
of motion and power of extension of the knees, functional
reach test, repeated sit-to-stand test, and the Chinese
Arthritis
Impact Measurement Scales 2.
Results: There was an
improvement in the median range of knee flexion
from 115° to 125° (P<0.01) and the median strength of the
quadriceps from 9 kg to 21 kg (P<0.001). The median score of
the
functional reach test increased from 20 cm to 28 cm (P<0.001)
and the repeated sit-to-stand test from 10 to 14 repetitions
(P<0.001). Also, there was an improvement in the mobility
level
(P<0.01), walking and bending ability of the trunk
(P<0.05),
levels of pain (P<0.01) and mood (P<0.01), and the total
score
(P<0.01) in the Chinese Arthritis Impact Measurement Scales
2.
Conclusions: Physiotherapist-designed
aquatic exercise has definite benefits
in terms of physical and psychosocial functioning, and should
be promoted as one of the strategies to enhance long-term
self-management of community elders with knee osteoarthritis.
New knowledge added by this
study
- This physiotherapist-designed aquatic exercise (PDAE) programme significantly improves knee functions, symptoms, and psycho-social functioning of the Hong Kong Chinese knee osteoarthritis (OA) sufferers.
- The PDAE programme was effective and feasible in community settings.
- This study showed that OA knee sufferers can improve in terms of knee symptoms and functioning by means of the PDAE programme used in a community setting.
- The findings support the application of PDAE programme as a form of long-term self-management for OA knee.
Introduction
Osteoarthritis of the knee (OA knee) is a
chronic painful and disabling condition affecting
elderly persons worldwide. Among all lower limb joints affected by
OA, affliction of the
knee is particularly common among the Hong Kong Chinese. A local
survey on persons
aged 50 years and above revealed that among men, 17% and 7% had
persistent knee pain
and a confirmed diagnosis of OA knee, respectively; the prevalence
rates in women were
higher, being 24% and 13%, respectively.1
Elderly Health Centres (EHCs) of the
Department of Health provide comprehensive
primary health care for persons aged 65 years and above. Among
attendees of EHCs, OA
knee contributes to approximately one third of all physiotherapy
referrals.2
Physiotherapy in the form of an exercise
prescription (eg hydrotherapy), other treatment
modalities (eg heat therapy, transcutaneous electrical
nerve stimulation), as well as the prescription of
mobility aids for improving ambulation are examples
of recommended non-pharmacological therapies for
the OA. These are in addition to patient education
and self-management programmes.3
There are many
studies documenting the efficacy and effectiveness
of aquatic exercises (or hydrotherapy programmes)
for reducing pain and improving function in patients
with OA or rheumatoid arthritis.4
5 6 7 8
When one
exercises in water, the buoyancy of water decreases
loading on lower limb joints. On the other hand, the
hydrodynamic resistance and turbulence helps to
strengthen muscles and increase proprioception and
balance. Hydrostatic pressure also helps to control
oedema in the immersed body parts.
This study aimed to examine the
effectiveness
and feasibility of a community-based aquatic exercise
programme for elders with OA knee. The programme,
a physiotherapist-designed aquatic exercise (PDAE),
was developed by the physiotherapists of the Elderly
Health Service (EHS) of the Department of Health.
Methods
Subjects
Subjects were recruited by convenience sampling of
the elders aged 65 years and above attending any one
of the four EHCs in Kowloon, Hong Kong.
Inclusion and exclusion criteria
Elders who were recruited had to have a clinical
diagnosis of OA knee made by EHC doctors, knee
pain for at least 3 years, and a self-perceived pain
level of at least ‘mild’ in the affected knee joint(s)
during the preceding 1 month.
Unstable heart disease, hypertension, or any
other medical contra-indication to mild-to-moderate
physical activity were grounds for exclusion.
Other exclusion criteria were physical barriers
to exercising in water, such as marked postural
deformity, blindness, or deafness; severe cognitive
impairment; depression not responding to treatment;
neurological diseases like Parkinson’s disease and
stroke; and inability to walk independently. Subjects
who had already received active interventions for
OA knee during the preceding 2 months or who had
scheduled knee operations in the following 6 months
were also excluded.
Interventions
The PDAE consisted of individual and group exercises
(Table 1), and was delivered twice a week for 10 weeks
in a public indoor swimming pool by registered
physiotherapists of the EHS.
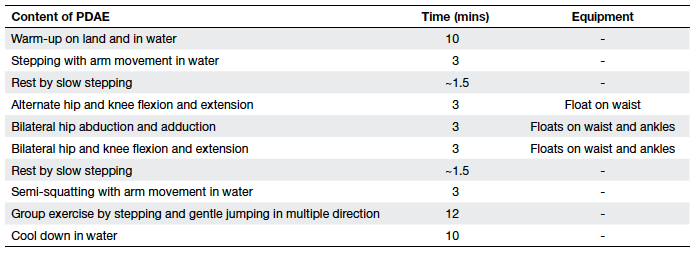
Table 1. Details of the physiotherapist-designed aquatic exercise (PDAE) programme
All subjects attended a health educational
seminar on OA knee and the PDAE before the
programme. This addressed the aetiology of OA
knee, advice on joint care, skills about coping with
daily living and self-help tips on symptomatic relief,
a rundown of the programme, and the preparation
required before undertaking the aquatic exercises.
Measurements
Characteristics of subjects
Measurements were carried out in the week
preceding and then following the intervention.
Demographic and co-morbidity data, including the
body mass index (BMI), were collected at baseline.
The history of knee pain and its management, self-reported
levels of involvement in household work
and exercise habits, and details about each subject’s
living environment were also documented.
Outcome measures
The outcome measures were:
(1) Self-reported changes in the use of analgesics (type and frequency of use).
(2) Changes in functional status, intensity and
pattern of pain, social activity, and level of
tension and mood, as measured by the Chinese
Arthritis Impact Measurement Scales 2 (CAIMS
2). The CAIMS 2 has been validated on Chinese-speaking
patients with arthritis9 (Table 2). Thirty
relevant items were extracted using CAIMS 2 in
the current study, and dealt with mobility, lower
limb functions, arthritis pain, and psychosocial
status.
(3) Functional exercise capacity was measured by
the 6-minute walk test, which measures the
maximum distance walked along a 50-metre
indoor course in 6 minutes.10 Learning effects
were minimised by testing each subject once
in the pre- and post-test, respectively and by a
3-month period between the tests.
(4) Lower limb strength and function were
measured using the dynamometer test of the
Nicholas Manual Muscle Tester (NMMT) and
the 30-second repeated sit-to-stand test. The
NMMT measures isometric quadriceps muscle
strength at 30° of knee flexion. The 30-second
repeated sit-to-stand test entails counting the
number of completed repetitions by the subject
in 30 seconds, and reflects composite functional
strength contributed by extension of the back
and legs.
(5) Standing balance was measured by the functional
reach test (FRT), which measures the maximum
displacement in horizontal distance that the
subjects can reach when they stand still. Scores
of less than 6 inches (15.2 cm) indicate limited
functional balance, 6 to 10 inches indicate a
moderate fall risk, and that of more than 10
inches (25.4 cm) indicate less fall risk.11
(6) The range of motion (ROM) of the knee joints was
measured by a goniometer with the subject in a
lying position. The range is one of the mediators for the improvement in overall knee function.
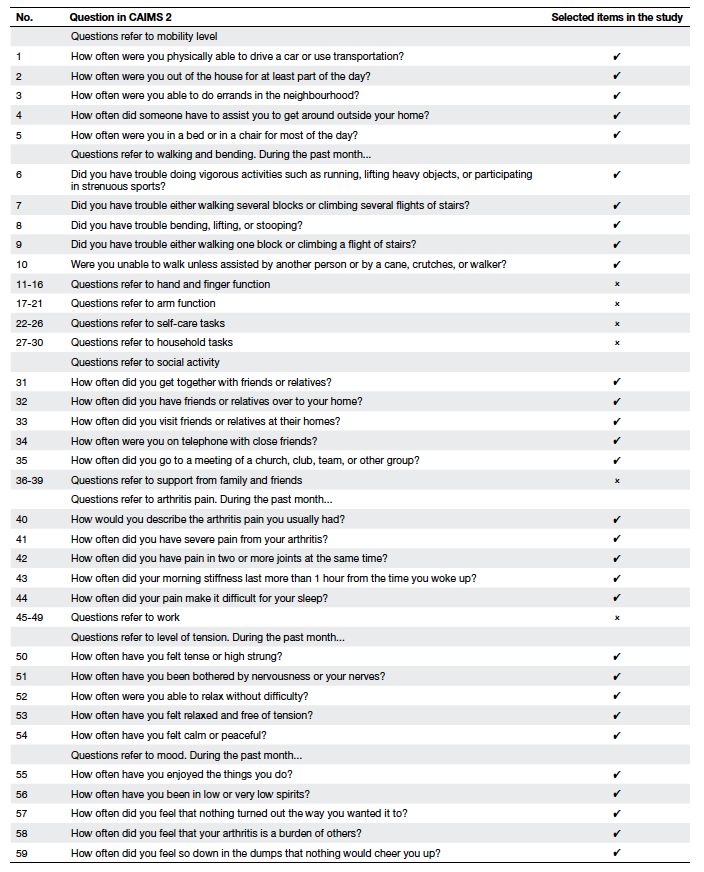
Table 2. The selected items for physiotherapist-designed aquatic exercise assessment out of the original Chinese Arthritis Impact Measurement Scales 2 (CAIMS 2) questionnaire9
Programme feasibility
The feasibility of running the PDAE programme in the
community was assessed as follows:
(a) Difficulties encountered and subjects’ concerns
during the recruitment;
(b) Attendance during programme implementation
and reasons of absence;
(c) Observation of subjects’ performance during the
PDAE programme; and
(d) Post-study programme evaluation including
subjects’ satisfaction and their opinion on future
service planning.
Statistical methods
Analyses were performed using the Statistical Package
for the Social Sciences (Windows version 10.0; SPSS
Inc, Chicago [IL], US). Differences in range of knee
movement, quadriceps strength, FRT, repeated
sit-to-stand test, 6-minute walk test, and CAIMS 2
scores before and after the PDAE were tested by the
Wilcoxon signed rank test, while the difference in
the use of analgesic medications for knee pain was
tested by McNemar’s test.
To detect a change of 20% in the pain and
physical functioning scales of CAIMS 2 with an α
level of 0.05 and 80% power, a sample size of 18 was
necessary according to the computer equation for
the Wilcoxon signed rank test. To allow for a dropout
rate of 20%, 22 subjects were recruited.
Results
Subject characteristics
There were 22 subjects, of whom 20 (15 female
and 5 male) completed the PDAE programme. Two
withdrew from the study—one due to personal and adjustment problems to water temperature,
while the other did not attend the post-programme
assessment. The mean (± standard deviation) age of
the subjects was 72 ± 2 years. In all, 35% of them were
illiterate and 50% had had a primary school education
(Table 3). Apart from OA of the knee, 65% of them
had other musculoskeletal problems. Moreover,
65% of the subjects lived in public housing and the
rest in private housing. All of them were involved in
managing household chores at moderate (60%) and
light (40%) intensity levels, and 90% of them had
direct lift access to their homes.
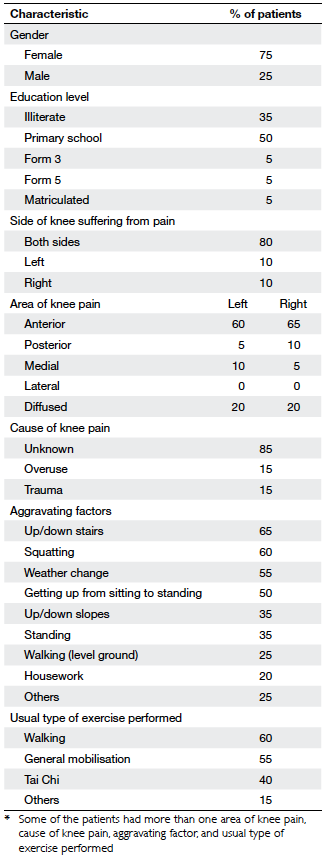
Table 3. Demographic and clinical characteristics of the sample*
Before participating in PDAE programme, 16 of
the subjects had pain in both knees and four in one
knee only. Specific causes of the knee pain were not
identified in 15 of them. Two subjects had pain in one
knee without specific cause but the other knee by
trauma. Two subjects had knee pain due to overuse.
Another subject had knee pain due to overuse and
trauma. The main aggravating factors were climbing
stairs, squatting, weather changes, and getting up
from a sitting to standing position (Table 3).
Nearly all the subjects (90%) undertook exercises
of different forms and intensity; 94% claimed to
exercise daily, 78% claimed to exercise 30 to 60 minutes per
day, and some (17%) claimed to exercise for more than
1 hour a day. Reported land-based exercises included
walking (60%), general mobilisation exercise (55%),
and Tai Chi (40%). Half of the subjects encountered
difficulties performing daily activities (brisk walking,
single-leg standing, squatting, getting up or standing
from squatting, or sitting on a low stool) due to knee
problems. Subject demographics and clinical features
are described in Table 3.
Body mass index
There was no significant difference in the subjects’
mean BMI before and after the PDAE programme
(26.6 vs 26.6 kg/m2; P=0.658).
Pain-relieving medications
Before PDAE, more than half of the subjects used
analgesic ointments/patches for self-management of
knee pain. Apart from medication, only one subject
exercised specifically to relieve pain and stiffness in
his knee. Three quarters of the subjects found their
self-management slightly effective and 20% found it
moderately effective.
After PDAE, the number of subjects taking pain-relieving
medications decreased (19 vs 4; P=0.004),
and the numbers relying on oral analgesics decreased
from four to one (Table 4).
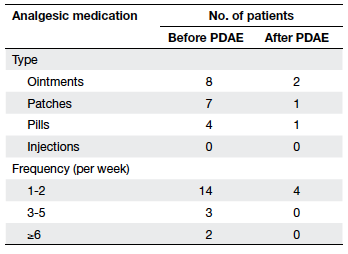
Table 4. Frequency and type of analgesic medication used before and after physiotherapist-designed aquatic exercise (PDAE) programme
Outcomes
According to observations by physiotherapists, subjects with knee swelling all experienced a
decrease (10 vs 0 knees; P=0.002). There was also a
decrease in the girth of the thigh (measured at 5 cm
above the base of patella in both knees) from a mean
of 40 cm to 39 cm (P<0.001), despite a substantial
increase of muscle strength (Tables 5 and 6).
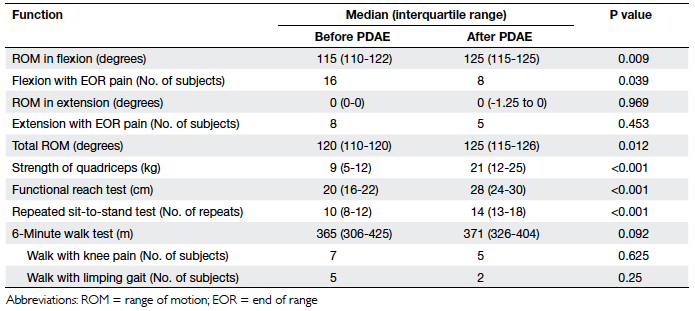
Table 5. Functional parameters of the knee before and after physiotherapist-designed aquatic exercise (PDAE) programme
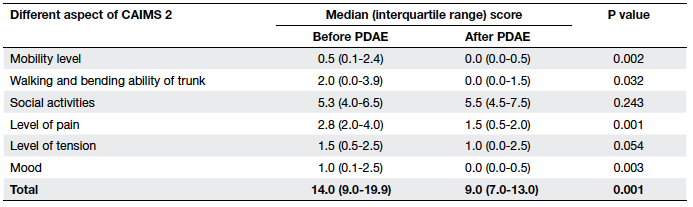
Table 6. The Chinese Arthritis Impact Measurement Scales 2 (CAIMS 2) scoring before and after physiotherapist-designed aquatic exercise (PDAE) programme
Owing to the small sample size and skewed
data distribution, medians and the non-parametric Wilcoxon signed rank test were used to compare
functional outcomes and CAIMS 2 scores.
The medians of the knee range of motion
increased from 115° to 125° (P<0.01) after the PDAE,
while those for total ROM increased from 120° to 125° (P<0.05). The number of subjects who got end-of-range
pain at flexion decreased from 16 to 8 (P<0.05).
There was also a marked improvement in the medians
for quadriceps strength from 9 kg to 21 kg (P<0.001),
FRT from 20 cm to 28 cm (P<0.001), and the repeated
sit-to-stand test from 10 to 14 repetitions (P<0.001).
There was a slight improvement in the median for the
6-minute walk test (Table 5).
There was a significant improvement in mobility
level, walking and bending ability of trunk, levels of
pain and mood, as well as the total score as measured
by CAIMS 2 (Table 6).
Discussion
Effectiveness of physiotherapist-designed aquatic
exercise programme
Osteoarthritis is associated with muscle atrophy,
reduced muscle strength, and decreased ROM.
Studies have shown that strength and ROM of women
with arthritis are often 70 to 85% that of women of
similar age without arthritis.12 Quadriceps weakness
is common among patients with OA knee, which is believed to be due to disuse atrophy, as patients tend
to unload the painful extremity.3 Osteoarthritis is a
common disorder in persons older than 65 years and
can significantly affect quality of life.13
The goal of the PDAE programme was to improve
knee function for the OA-affected knee. In this study,
the intervention was associated with a reduction in
knee pain, improved strength of knee extensors,
improved knee ROM, and overall body balance; all of
which were confirmed by improvements in the sit-to-stand
test.
The advantage of exercising in an aquatic
environment is that in comparison to usual weight-bearing
exercises, water buoyancy decreases stress
on the lower limb joints and surrounding muscles,
which provides the ideal medium for pain and
stiffness relief from arthritis. Turbulence and its
dynamic resistance is another property that can
strengthen all muscle groups surrounding the knee,
and improve proprioception and body balance.5
The results of this study were concordant
with the mentioned benefits of the multi-direction
resistance provided by the water environment, such
that PDAE strengthens the quadriceps effectively.
The increased muscle strength around affected
joints is a clinically important outcome, as muscles
provide shock-absorbing capacity and joint stability
to help preserve the diseased joint.4 The decrease
in knee joint girth might be explained by reduced
swelling and the proximal lift from muscle bulk of the
quadriceps and hamstrings due to improved muscle
tone.
Moreover, the turbulence of water not only
provides resistance but also a multi-directional
balance challenge. The aquatic environment enables
subjects with intrinsic fall risk factors to exercise safely
in functional positions. In this study, improvements
in trunk movement ability were also noted in the
CAIMS 2 questionnaire. The above factors may be the
main reasons for improvement in functional balance.
In this study, the medians of the subjects’ FRT test
results after PDAE improved from a moderate level
of fall risk to a less risky level. This change concurs
with Simmons and Hansen’s findings,13 whereby
greater improvement in functional reach occurred
in subjects who had exercised in an aquatic
environment. Challenges to balance in an aquatic
environment appear to improve dynamic standing
balance on land. This is further supported by motor
learning literature, where learners demonstrated the
ability to apply what they had learnt from different
practice conditions and/or movement skills.14
Standing balance training, if sufficiently dynamic
in nature, may also improve the performance of
functional activities that combine elements of
dynamic balance and overall mobility.14 Overall, the
functional movement of the knee reflected by the sit-to-stand test also improved.
The improvements in the mentioned domains
of knee function were contributed to by decreased
knee pain after the programme. In reference to the
self-management of the knee symptoms, subjects
mainly used analgesic ointment and patches. Before
the PDAE programme, they might not have realised
that exercise was an effective means of improving
their knee pain and function. The PDAE programme
benefits subjects via performance of suitable
exercise so that they are less dependent on drugs
and hence drug-induced adverse effects can be
reduced.
Moreover, the present study showed that
PDAE had added benefits on both the physical
and psychological aspects of patients with OA
knee. Group interaction and socialisation resulting
from the interventions may also have influenced
psychological domains positively.13 Our results were
consistent with findings of other investigators, who
noted improvements in clinically active joint function
after hydrotherapy but not after a land-based exercise
programme.5 Although there was a deterioration in
the medians of the sub-score of social activities in
CAIMS 2 (P=0.243), this might have been because
the latter questionnaire focused on the frequency of
getting in touch with friends or relatives, rather than
about social activities resulting from the intervention.
Although nearly all subjects undertook
exercise and on a daily basis before the programme,
there was ample scope for improvement in the
physical domains for their knees. This might suggest
that different types of exercise, including aquatic
exercise, should be performed as part of any
exercise programme. Besides, measures should be
introduced to reduce risk factors for OA knee, such
as weight control by means of diet, exercise, and
education.
Feasibility of physiotherapist-designed aquatic
exercise programme
The observed positive effects and the high (96%)
overall attendance rate showed that the PDAE
programme was highly acceptable even for a
community-dwelling elderly population. This
compares very favourably to an attendance rate of
40 to 55% usually achieved in exercise programmes
for persons with arthritis.15 Satisfactory compliance
could be because those who joined the programme
could be non-swimmers, and the programme was
relatively short in duration (10 weeks). Moreover, it
was conducted during relatively warm months in a
training pool provided with temperature control by
radiators (room temperature ranged between 19°C and
29°C), resulting in an environment warm enough for
elders to exercise. Finally, there was good rapport between the subjects and the physiotherapists.
Timely advice, support, and encouragement by the
physiotherapists might also encourage the subjects to
adhere to the programme schedule. Although these
components were not evaluated in the programme,
one might speculate that emphasis on these aspects
helped attain the high degree of compliance.
During the recruitment period and
implementation of the PDAE, no difficulties or
adverse effects were encountered. The subjects
found the exercise intensity of the PDAE suitable
(mean rate of perceived exertion = 3.3 ± 1.3). Also, all
the participants were satisfied with the programme
and accepted its benefits, particularly as the PDAE
was feasible for implementation in public swimming
pool within a community setting.
Limitation
A major limitation of this study was the lack of a
control group. Therefore, there was no yardstick
for comparing the effects of the PDAE with no
intervention. Secondly, comparison of outcome
measures before and after PDAE could have been
influenced by co-interventions (eg use of massage,
improvements in posture during daily activities,
performance of other types of muscle-strengthening exercises). Moreover, the subjects recruited from
EHCs might well be more motivated and health
conscious than others. Thirdly, the outcomes were
measured without blinding, such that there was
always some measurement bias. Finally, the relatively
small sample size and recourse to convenience
sampling may have conferred imprecision and bias.
The benefits of aquatic exercise were already
well established in other studies. Our study
confirmed its effectiveness for OA knee, specifically
in a public swimming pool within a community
setting. Furthermore, the experience we gained
was valuable for the conduct of any future aquatic
exercise programme in the community.
Conclusions
The PDAE showed appreciable benefits in terms of
reducing knee pain, and improving knee function,
body balance, and the psychosocial health of elders
with OA knee, including non-swimmers. Populations
with OA knee problems and with or without those
related to weight-bearing exercise benefited from
aquatic exercise. The results justify continuing
investment in aquatic exercise programmes as one of
the strategies to enhance long-term self-management
for elders with chronic OA knee.
References
1. The Chinese University of Hong Kong. Osteoarthritis in
Hong Kong Chinese—Prevalence, aetiology and prevention
[press release]; 2001. Available from: www.cuhk.hk/ipro/010306e.htm. Accessed Sep 2004.
2. Elderly Health Service, Department of Health, Hong Kong.
Annual Report 2002.
3. American College of Rheumatology Subcommittee on
Osteoarthritis Guidelines. Recommendations for the
medical management of osteoarthritis of the hip and knee:
2000 update. Arthritis Rheum 2000;43:1905-15. Crossref
4. Foley A, Halbert J, Hewitt T, Crotty M. Does hydrotherapy
improve strength and physical function in patients with
osteoarthritis—a randomized controlled trial comparing
a gym-based and a hydrotherapy-based strengthening
program. Ann Rheum Dis 2003;62:1162-7. Crossref
5. Geytenbeek J. Evidence for effective hydrotherapy.
Physiotherapy 2002;88:514-29. Crossref
6. Hall J, Skevington SM, Maddison PJ, Chapman K. A
randomized and controlled trial of hydrotherapy in
rheumatoid arthritis. Arthritis Care Res 1996;9:206-15. Crossref
7. Minor MA, Hewett JE, Webel RR, Anderson SK, Kay DR.
Efficacy of physical conditioning exercise in patients with
rheumatoid arthritis and osteoarthritis. Arthritis Rheum
1989;32:1396-405. Crossref
8. Wyatt FB, Milam S, Manske RC, Deere R. The effects of
aquatic and traditional exercise programs on persons with knee osteoarthritis. J Strength Cond Res 2001;15:337-40. Crossref
9. Chu EM, Chiu KY, Wong RW, Tong WM, Lau CS. Translation
and validation of Arthritis Impact Measurement Scales 2 into
Chinese: CAIMS 2. Arthritis Rheum 2004;51:20-7. Crossref
10. Enright PL, McBurnie MA, Bittner V, et al. The 6-min walk
test: a quick measure of functional status in elderly adults.
Chest 2003;123:387-98. Crossref
11. Ducan PW, Studenski S, Chandler J, Prescott B. Functional
reach: predictive validity in a sample of elderly male
veterans. J Gerontol 1992;47:M93-8. Crossref
12. Ekdahl C, Broman G. Muscle strength, endurance, and
aerobic capacity in rheumatoid arthritis: a comparative
study with healthy subjects. Ann Rheum Dis 1992;51:35-40. Crossref
13. Simmons V, Hansen PD. Effectiveness of water exercise on
postural mobility in the well elderly: an experimental study
on balance enhancement. J Gerontol A Biol Sci Med Sci
1996;51:M233-8. Crossref
14. Rose DJ, Clark S. Can the control of bodily orientation be
significantly improved in a group of older adults with a
history of falls? J Am Geriatr Soc 2000;48:275-82.
15. Dexter PA. Joint exercises in elderly persons with
symptomatic osteoarthritis of the hip or knee. Performance
patterns, medical support patterns, and the relationship
between exercising and medical care. Arthritis Care Res
1992;5:36-41. Crossref