© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
PICTORIAL MEDICINE
Eyelash trichomegaly induced by erlotinib for
metastatic lung cancer
Julia YY Chan, AFCOphth HK, MRCSEd (Ophth)1,2; Tracy YT Kwok, FCOphth HK, FHKAM (Ophthalmology)1,2; Hunter KL Yuen, FRCOphth, FRCSEd1,2
1 Department of Ophthalmology and Visual Sciences, The Chinese University of Hong Kong, Hong Kong
2 Hong Kong Eye Hospital, Hong Kong
Corresponding author: Dr Julia YY Chan (cyyj717@gmail.com)
 Full
paper in PDF
Full
paper in PDF
A 65-year-old Chinese woman was referred to the
ophthalmology clinic complaining of grittiness in
both eyes for 1 month. She had been diagnosed with
stage IV metastatic pulmonary adenocarcinoma
with positive mutation in epidermal growth factor
receptor (EGFR) gene (L858R) and had been
prescribed erlotinib 4 months previously as palliative
treatment (Table).
Table. Timeline of the patient
Physical examination revealed bilateral long
thick curly eyelashes (Figs 1 and 2) affecting all four
eyelids. A papulopustular rash over the periocular
region was also evident. The patient denied use of
topical prostaglandin analogue for either medical or
cosmetic use. A diagnosis was made of drug-induced
trichomegaly. Corneal punctate epithelial erosion
as a result of the misdirected lashes was treated
symptomatically with regular epilation and topical
lubricants.
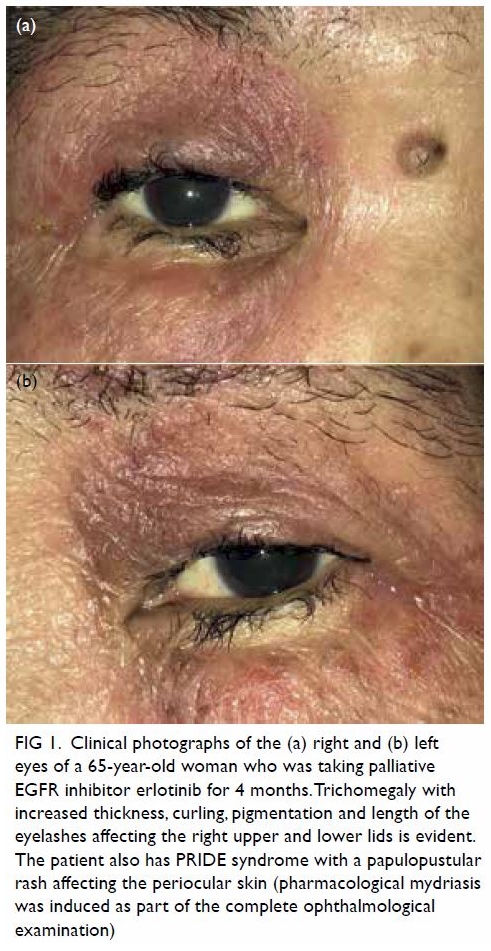
Figure 1. Clinical photographs of the (a) right and (b) left eyes of a 65-year-old woman who was taking palliative EGFR inhibitor erlotinib for 4 months. Trichomegaly with increased thickness, curling, pigmentation and length of the eyelashes affecting the right upper and lower lids is evident. The patient also has PRIDE syndrome with a papulopustular rash affecting the periocular skin (pharmacological mydriasis was induced as part of the complete ophthalmological examination)
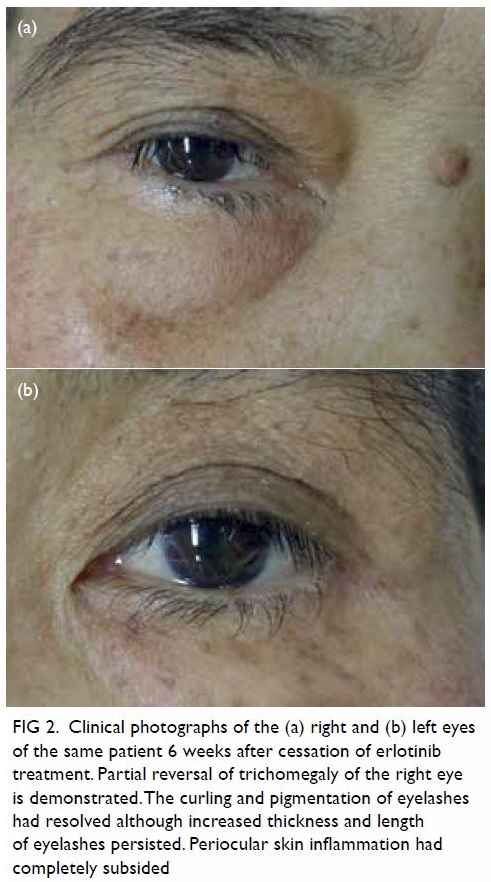
Figure 2. Clinical photographs of the (a) right and (b) left eyes of the same patient 6 weeks after cessation of erlotinib treatment. Partial reversal of trichomegaly of the right eye is demonstrated. The curling and pigmentation of eyelashes had resolved although increased thickness and length of eyelashes persisted. Periocular skin inflammation had completely subsided
Upon follow-up, gradual partial reversal of
trichomegaly was evident at 6 weeks after erlotinib
cessation. There was also improvement of the
periorbital papulopustular rash. The reversal of
trichomegaly after EGFR inhibitor cessation is
not well documented in the literature. This case
illustrates the presentation and partial resolution of
drug-induced trichomegaly.
Eyelash trichomegaly is a rare condition
characterised by increase in length, thickness,
pigmentation, and curling of the eyelashes. The
eyelash follicle, just as the scalp hair follicle,
undergoes the cycle of anagen, catagen, and telogen
phase. The anagen phase of eyelashes (ie, the growth
phase) typically spans 8 weeks in Asian patients and
occurs in 18% of eyelashes at any given time.1
Drug-induced trichomegaly is the most
common form of trichomegaly to present in a general
ophthalmology setting. Prostaglandin analogues such as latanoprost and bimatoprost, although
commonly used as antiglaucomatous drugs, are well
known for their side-effect of eyelash trichomegaly.
The effect is due to up-regulation of prostaglandin
E2, D2 receptor expressed in hair follicles.2
The occurrence of EGFR inhibitor–induced
trichomegaly is seen less often but is not uncommon
in the ophthalmology setting. It has been postulated
that EGFR inhibitors inactivate the nuclear factor
of activated T-cells. This leads to activation of stem
cell bulge and suprabulbar region of the eyelash hair
follicles.3 In a typical course, trichomegaly develops
between the second and fifth month of EGFR
inhibitor treatment.4 An Asian study reported that
2% of patients prescribed EGFR inhibitor treatment
had trichomegaly.5 The EGFR inhibitor is also well
known to cause a series of cutaneous adverse effects
known as the PRIDE syndrome (papulopustules
and/or paronychia, regulatory abnormalities of
hair growth, itching, and dryness).6 In this case, the
patient exhibited PRIDE syndrome affecting the periocular skin as demonstrated in Figures 1 and 2.
Trichomegaly is a benign condition, but long
misdirected lashes may lead to corneal punctate
epithelial erosion and corneal abrasion. Frequent
trimming, epilation, and topical lubricants serve as
first-line treatment. Electro-epilation or cryoablation
directed at the affected hair follicles may be
considered in instances of recurrent misdirected
lashes with corneal complications such as infective
corneal ulcer.
This case highlights the clinical course of EGFR
inhibitor–induced trichomegaly upon cessation
of drug therapy, which is not well documented in
the literature. Partial reversal of trichomegaly was
achieved after stopping erlotinib for 6 weeks. It is
evident that the time required for trichomegaly
resolution follows the typical eyelash follicle cycle.
Author contributions
All authors contributed to the design, acquisition of data,
analysis of data, drafting of the manuscript, and critical
revision of the manuscript for important intellectual content.
All authors had full access to the data, contributed to the
study, approved the final version for publication, and take
responsibility for its accuracy and integrity.
Conflicts of interest
As an adviser of the journal, HKL Yuen was not involved in the peer review process. Other authors have disclosed no
conflicts of interest.
Funding/support
This pictorial medicine received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
The patient was treated in accordance with the Declaration of Helsinki. The patient provided written informed consent for
the treatment/procedures, and consent for publication.
References
1. Na JI, Kwon OS, Kim BJ, et al. Ethnic characteristics of
eyelashes: a comparative analysis in Asian and Caucasian
females. Br J Dermatol 2006;155:1170-6. Crossref
2. Colombe L, Michelet JF, Bernard BA. Prostanoid receptors in anagen human hair follicles. Exp Dermatol 2008;17:63-
72. Crossref
3. Dalal A, Sharma S, Kumar A, Sharma N. Eyelash
trichomegaly: a rare presenting feature of systemic lupus
erythematosus. Int J Trichology 2017;9:79-81. Crossref
4. Jeon SH, Ryu JS, Choi GS, et al. Erlotinib induced trichomegaly of the eyelashes. Tuberc Respir Dis (Seoul)
2013;74:37-40. Crossref
5. Chanprapaph K, Pongcharoen P, Vachiramon V.
Cutaneous adverse events of epidermal growth factor
receptor inhibitors: A retrospective review of 99 cases. Indian J Dermatol Venereol Leprol 2015;81:547. Crossref
6. Lacouture ME, Lai SE. The PRIDE (Papulopustules
and/or paronychia, Regulatory abnormalities of hair
growth, Itching, and Dryness due to Epidermal growth
factor receptor inhibitors) syndrome. Br J Dermatol
2006;155:852-4. Crossref