© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
REMINISCENCE: ARTEFACTS FROM THE HONG KONG MUSEUM OF MEDICAL SCIENCES
Sharman’s kymographic tubal insufflation apparatus
Pamela Leung, FHKAM (Obstetrics and Gynaecology)
Director, Hong Kong Museum of Medical Sciences Society
 Full
paper in PDF
Full
paper in PDF
The tubal insufflation of oxygen to demonstrate the patency of the Fallopian tubes was first described by Dr Isidor Clinton Rubin in 1920.1 Later, Rubin advocated the use of carbon dioxide for insufflation because it is more rapidly absorbed from the peritoneal cavity. The original apparatus used was very simple, consisting of a cannula for introduction into the cervix, an oxygen or carbon dioxide cylinder, and the necessary connections. In 1928, Rubin described a kymographic method to demonstrate the pressure at which the gas escaped through the tubes.2
In 1940, Professor Gordon King, Professor of Obstetrics & Gynaecology at The University of Hong Kong, described in great detail his analysis of the results of 635 insufflations, which he performed using the kymographic method.3
In 1944, Dr Albert Sharman of the Royal Samaritan Hospital for Women in Glasgow, the United Kingdom, first reported his kymographic tubal insufflation apparatus in the British Medical Journal.4 Early models were manufactured by Kelvin, Bottomley & Baird Ltd (United Kingdom), which later became Kelvin Hughes Limited (United Kingdom). It is one of these later models that was donated to the Hong Kong Museum of Medical Sciences by Dr YK Tsao (Fig).
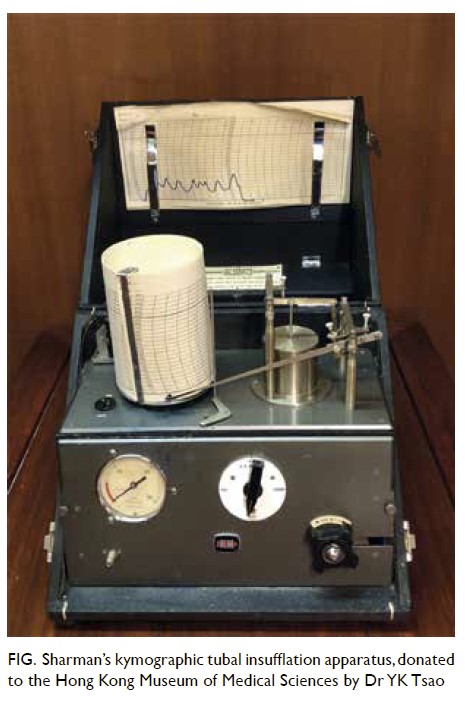
Figure. Sharman’s kymographic tubal insufflation apparatus, donated to the Hong Kong Museum of Medical Sciences by Dr YK Tsao
Tubal insufflation is a day procedure that does not need hospital admission. With the patient in the lithotomy position, the vulva is cleansed with antiseptic solution and suitably draped. The vaginal wall and cervix are exposed with a self-retaining speculum and then cleansed with antiseptic solution. After a thorough digital vaginal examination, the anterior lip of the cervix is grasped with a single-toothed Vulsellum forceps and the length and direction of the uterine cavity is determined by the passage of a uterine sound. A uterine cannula with a rubber cone (Rubin’s cannula) is then passed through the cervix so that the rubber cone comes into firm contact with the external cervical os. Firm upward pressure on the cannula together with downward traction on the Vulsellum forceps ensures that gas will not escape from the cervical os. The opening of the uterine cannula is then connected to the insufflation apparatus via rubber tubing. The valve of the apparatus is opened to allow carbon dioxide to flow into the system. The pressure achieved within the system is marked by a pen on recording paper previously mounted on the slowly rotating drum. The maximum pressure recorded must not exceed 250 mm Hg, at which time, the flow of carbon dioxide must be arrested. At the same time, an assistant will auscultate the right and left iliac fossae with a stethoscope for signs of gas passing into the peritoneal cavity via the fimbriated ends of the Fallopian tubes. Patency of the tubes is indicated when the pressure falls during gas insufflation, usually between 75 mm Hg and 125 mm Hg. As the pressure falls, well-marked oscillations may be seen on the graph due to rhythmic contractions of the Fallopian tubes. Blocked tubes are indicated when the pressure does not fall even when pressure reaches the maximum of 250 mm Hg and the flow of carbon dioxide is arrested. In cases of tubal stenosis, after stoppage of gas flow upon reaching 250 mm Hg, the pressure may slowly fall, but without oscillations.
Nowadays, tubal insufflation of carbon dioxide has been supplanted by hysterosalpingogram in which a radiopaque dye is injected through the cervix and a radiological image is taken to determine tubal patency. Alternatively, the pelvic organs may be visualised by means of a laparoscope inserted into the peritoneal cavity after it has been distended by carbon dioxide. Tubal patency is then demonstrated by chromotubation, whereby a solution of methylene blue or indigo carmine is injected through the cervix by an assistant and the blue dye is seen flowing from the fimbriated ends of the Fallopian tubes.
References
1. Rubin IC. Landmark Article April 10, 1920: Nonoperative determination of patency of fallopian tubes in sterility. Intra-uterine inflation with oxygen, and production of an artificial pneumoperitoneum. Preliminary report. By I.C. Rubin. JAMA 1983;250:2358. Crossref
2. Rubin IC. Tubal patency: clinical study in 650 cases of sterility by method of peruterine insufflation combined with kymograph. JAMA 1928;90:99-106. Crossref
3. King G. Utero-tubal insufflation: An analysis of the results of 635 insufflations performed by the kymographic method. HKU Caduceus 1940;19:161-88.
4. Sharman A. Apparatus for utero-tubal insufflation. Br Med J 1944;1:460.