Hong
Kong Med J 2019 Aug;25(4):287–94 | Epub 12 Aug 2019
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
ORIGINAL ARTICLE
Pathogens in preterm prelabour rupture of membranes and
erythromycin for antibiotic prophylaxis: a retrospective analysis
YY Li, MB, ChB; CW Kong, MB, ChB, MSc; William WK
To, MD
Department of Obstetrics and Gynaecology, United
Christian Hospital, Kwun Tong, Hong Kong
Corresponding author: Dr CW Kong (melizakong@gmail.com)
 Full
paper in PDF
Full
paper in PDF
Abstract
Introduction: Many authoritative
guidelines recommend prescribing erythromycin as antibiotic prophylaxis
in patients with preterm prelabour rupture of membranes (PPROM). This
study evaluated the spectrum of pathogens in PPROM and assessed the
effectiveness of erythromycin prophylaxis.
Methods: This retrospective
study enrolled pregnant patients who were diagnosed with PPROM and who
delivered at ≥24 weeks of gestation in an obstetric unit from 2013 to
2017. Pathogens isolated from maternal, placental, and neonatal
specimens were analysed; their sensitivity profiles to various
antibiotics were recorded. Neonatal outcomes were also
evaluated.
Results: The overall incidence
of PPROM was 2.63%. Gram-positive bacteria were cultured in 18.4% of
PPROM patients (most frequent: Group B Streptococcus [GBS;
14.6%]); Gram-negative bacteria were cultured in 12.8% of PPROM patients
(most frequent: Escherichia coli [8.0%]). Both Gram-positive and
Gram-negative bacteria were significantly associated with early-onset
neonatal sepsis (P=0.036 and P=0.001). In analyses stratified by
bacterial species, E coli was significantly associated with
early-onset neonatal sepsis (P=0.004), whereas GBS was not (P=0.39).
Gram-positive bacteria had high rates of resistance to common
antibiotics: 42.2% of GBS and 50.0% of Enterococcus and other Streptococcus
bacteria were resistant to erythromycin. Escherichia coli had
high rates of resistance to ampicillin (70.3%) and gentamicin (33.3%);
rates of resistance to co-amoxiclav (3.6%) and intravenous cefuroxime
(14.0%) were low.
Conclusion: Gram-positive and
Gram-negative bacteria were found in 29.1% of PPROM patients.
Administration of erythromycin alone was insufficient to control these
bacteria in 67.7% of patients with positive cultures.
New knowledge added by this study
- Gram-positive and Gram-negative bacteria were found in 29.1% of patients with preterm prelabour rupture of membranes (PPROM), and the presences of these bacteria were significantly associated with the development of early-onset neonatal sepsis.
- Erythromycin alone is insufficient to control the growth of Gram-positive and Gram-negative bacteria in patients with PPROM. In particular, Escherichia coli and Group B Streptococcus isolates showed high rates of resistance to erythromycin.
- Based on the increase in Gram-negative bacteria and the association of these bacteria with early-onset neonatal sepsis, intravenous cefuroxime (a second-generation cephalosporin) is proposed for use as antibiotic prophylaxis, in combination with erythromycin, in patients with PPROM.
Introduction
Preterm prelabour rupture of membranes (PPROM)
occurs in 2.0% to 3.5% of pregnancies and contributes to 30% to 40% of all
preterm births.1 Importantly, PPROM
is directly associated with preterm labour, prematurity, chorioamnionitis,
maternal and neonatal infections, and adverse maternal and neonatal
outcomes.2 Patients with PPROM
reportedly have a higher rate of abnormal microbial colonisation of the
genital tracts than patients without PPROM; the prevalence of positive
amniotic-fluid cultures in PPROM patients is approximately 32% to 35%.1 Administration of antibiotics in PPROM patients has
been shown to significantly reduce clinical chorioamnionitis; delay the
onset of delivery; decrease neonatal infection; and reduce the use of
surfactant, oxygen therapy, and abnormal neonatal cerebral ultrasound
prior to discharge from hospital.3
A randomised controlled trial published in 1997
showed that the use of erythromycin and ampicillin as antibiotic
prophylaxis in PPROM patients could significantly reduce neonatal
morbidity.4 In 2001, the landmark
randomised controlled trial ORACLE 1 showed that the use of erythromycin
could significantly prolong pregnancy in PPROM patients and could improve
neonatal outcomes.1 Based on the
above two trials, many authoritative guidelines recommend prescribing
erythromycin with or without ampicillin for PPROM patients, including
guidelines from the Royal College of Obstetricians and Gynecologists,5 the American College of Obstetricians and
Gynecologists,6 the Society of
Obstetricians and Gynaecologists of Canada,7
and the Royal Australian and New Zealand College of Obstetricians and
Gynaecologists.8
However, more recent studies have found that
colonisation by Gram-negative bacteria, especially Escherichia coli,
has been increasing in PPROM patients, such that these bacteria constitute
a significant proportion of all pathogens involved in cases of PPROM and
early-onset neonatal sepsis.9 10 Because the above two trials were conducted nearly 20
years ago, the objective of this study was to re-evaluate the pathogens
involved in PPROM and characterise their respective sensitivity profiles
to guide the appropriate choice of antibiotics used for optimal control,
and to assess whether erythromycin remains an effective antibiotic to
control these pathogens in PPROM patients.
Methods
This was a retrospective analysis of a cohort of
all pregnant patients who were diagnosed with PPROM and who delivered at
≥24 weeks of gestation in United Christian Hospital from 1 January 2013 to
31 December 2017. These patients were identified and retrieved from the
labour ward registry. Diagnoses of PPROM were made based on clinical
history and speculum examination to determine the presence of liquid
leaking from the cervical os; ultrasound was performed when necessary to
aid the diagnosis of PPROM. In accordance with our department protocol,
all patients who were diagnosed with PPROM underwent microbiological
investigation, including high vaginal swab and mid-stream urine for
bacterial culture, and low vaginal swab and rectal swab for Group B Streptococcus
(GBS) culture. Maternal blood culture was performed if maternal fever or
signs of acute chorioamnionitis were observed. Microbiological
investigation was repeated when clinically indicated. All patients who
were diagnosed with PPROM were administered oral erythromycin 250 mg, 4
times per day for 10 days, unless labour was established; patients at
<35 weeks of gestation were administered intramuscular dexamethasone to
enhance fetal lung maturity, in accordance with the NICE guideline adopted
by the Royal College of Obstetricians and Gynaecologists.5 Conservative management was adopted for patients at
<34 weeks of gestation, unless there was evidence of acute
chorioamnionitis or preterm labour was established. Possible induction of
labour was discussed with patients at ≥34 weeks of gestation. Caesarean
section was performed in accordance with obstetric indications.
Erythromycin was changed to another appropriate antibiotic if culture
results demonstrated the presence of erythromycin-resistant bacteria. If a
patient had spontaneous or induced labour, intravenous benzyl penicillin
was administered to control GBS until the baby was delivered. For all
PPROM patients, placental swabs were sent for bacterial culture and the
placentae were sent for histology examination after delivery. All neonates
were assessed by paediatricians after birth and appropriate neonatal
cultures were taken as indicated. Regardless of the presence of positive
bacterial cultures, neonates were diagnosed with early-onset neonatal
sepsis if they had signs of systemic infection within 72 hours after
birth; these signs included unstable body temperature, lethargy or
irritability, feeding intolerance, respiratory distress, tachycardia or
hypotension, metabolic changes (eg, glucose level and acidosis),
neutropenia, or increased acute-phase reactants (eg, C-reactive protein).
The demographic and clinical data of the pregnant
patients and their neonates were retrieved from a comprehensive obstetric
database and the Clinical Management System of the Hospital Authority. The
SPSS (Windows version 20.0; IBM Corp, Armonk [NY], United States) was used
for data entry and analysis. Continuous variables were analysed by t
test, whereas discrete variables were analysed by the Chi squared test or
Fisher’s exact test. A P value of <0.05 was considered to be
statistically significant. The STROBE (Strengthening the Reporting of
Observational Studies in Epidemiology) guidelines were followed in the
preparation of this article.11
Results
In total, there were 21 047 pregnancies with 21 375
babies delivered during the study period, including 324 pairs of twins and
two sets of triplets. The incidence of PPROM was 2.63% (553/21 047),
including 39 pairs of twins. The demographic data and pregnancy outcomes
of patients with and without PPROM are shown in Table 1. Advanced maternal age, primiparity, and
multiple pregnancies were more common among patients in the PPROM group
than among patients in the non-PPROM group. Patients with PPROM delivered
earlier (34.1 vs 38.8 weeks; P<0.0001) and had lower birthweight babies
(2260 g vs 3142 g; P<0.001) than patients without PPROM. The incidence
of neonatal death was higher in the PPROM group than in the non-PPROM
group (1.4% vs 0.1%; P<0.001), whereas the incidence of stillbirth did
not significantly differ between the two groups (0.3% vs 0.3%; P=0.73).
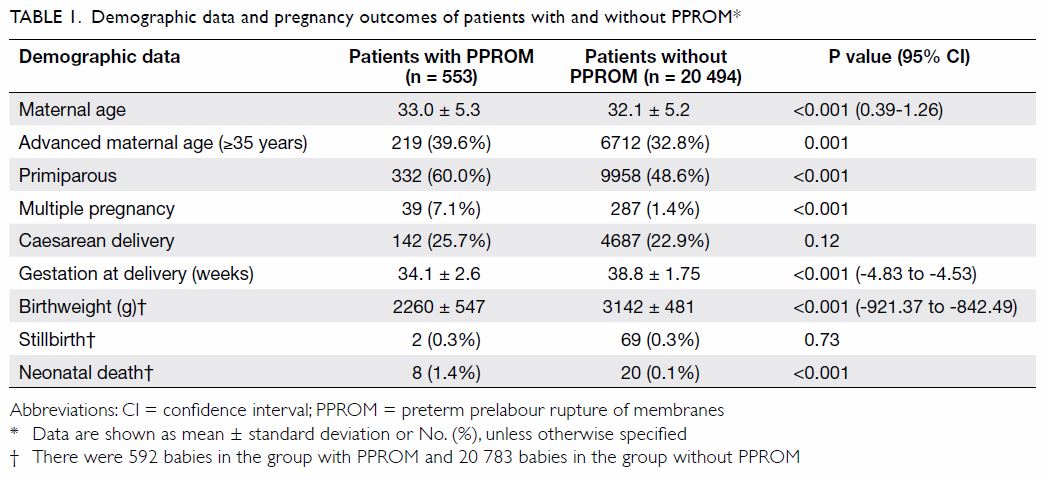
Table 1. Demographic data and pregnancy outcomes of patients with and without PPROM
The outcomes of patients with PPROM and the types
of bacteria cultured from maternal, placental, and neonatal specimens are
shown in Table 2. Gram-positive bacteria were found in 18.4%
of PPROM patients, among which GBS was the most common (14.6%);
Gram-negative bacteria were found in 12.8% of PPROM patients, among which
E coli (8.0%) was the most common. In addition, anaerobes were
found in 1.8% of PPROM patients. Although 19.2% of placental histology
specimens showed evidence of chorioamnionitis or funisitis, only 4.7% of
PPROM patients were clinically diagnosed with acute chorioamnionitis.
However, early-onset neonatal sepsis was diagnosed in 10.8% of newborns.
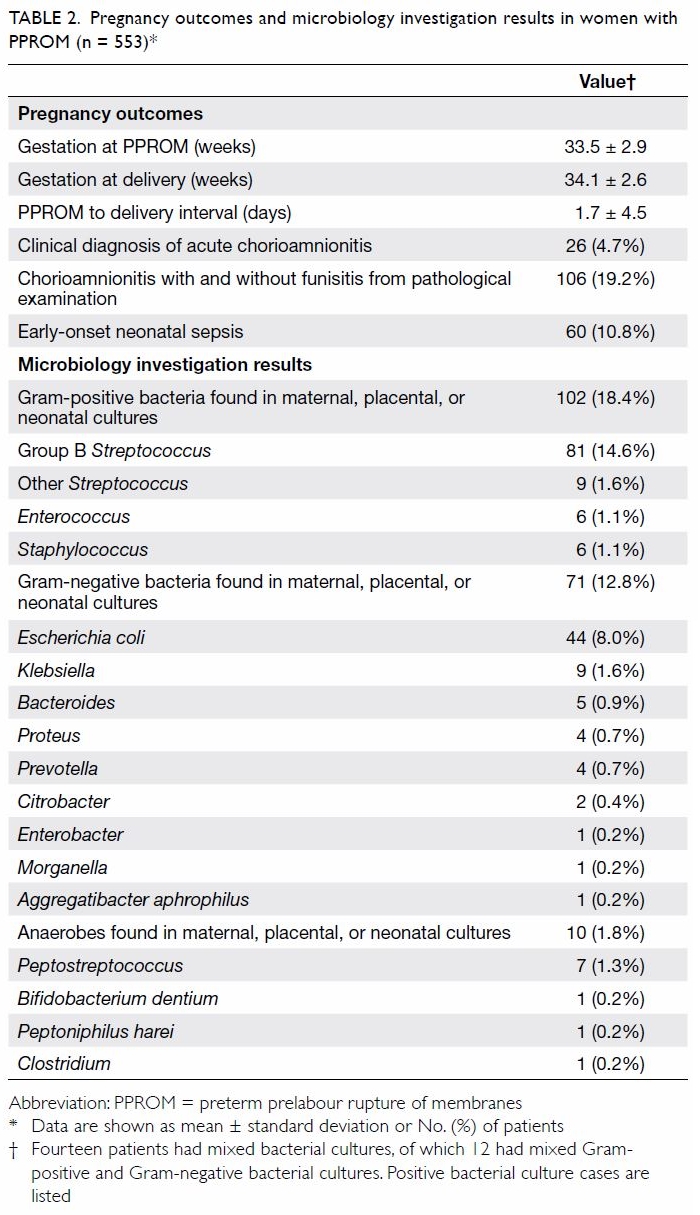
Table 2. Pregnancy outcomes and microbiology investigation results in women with PPROM (n = 553)
Preterm prelabour rupture of membranes occurred
earlier in gestation in patients with early-onset neonatal sepsis than in
those without neonatal sepsis (31.1 vs 34.2 weeks; P<0.001), and the
PPROM to delivery interval was longer in patients with early-onset
neonatal sepsis (3.7 vs 1.5 days; P<0.001). The presences of
Gram-positive bacteria and Gram-negative bacteria were significantly
associated with the development of early-onset neonatal sepsis (P=0.036
and P=0.001, respectively), whereas the presence of anaerobes was not
(P=0.08). In addition, the presence of E coli was significantly
associated with the development of early-onset neonatal sepsis (P=0.004),
whereas the presence of GBS was not (P=0.39) [Table 3].
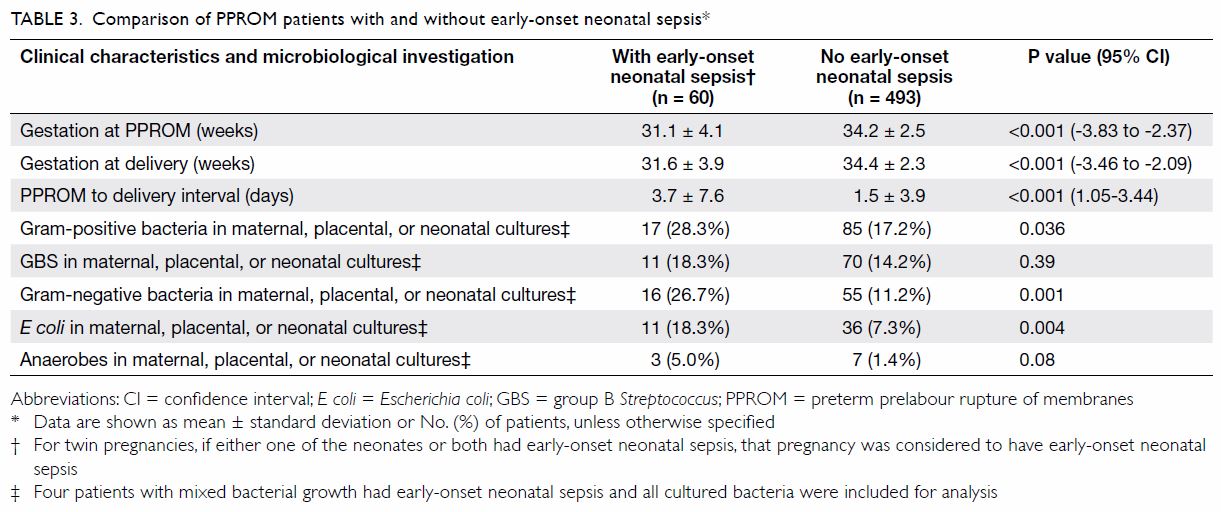
Table 3. Comparison of PPROM patients with and without early-onset neonatal sepsis
The rates of resistance of Gram-positive bacteria
and Gram-negative bacteria to various antibiotics are shown in Tables
4 and 5, respectively. All GBS isolates were sensitive to
penicillin, but 42.2% of them were resistant to erythromycin; other Streptococcus
and Enterococcus isolates also showed resistance to erythromycin
(50% of each group). Escherichia coli isolates demonstrated high rates of
resistance to ampicillin (70.3%) and gentamicin (33.3%), but low rates of
resistance to co-amoxiclav (3.6%) and intravenous cefuroxime (14.0%).
Notably, our laboratory did not routinely perform sensitivity testing of E
coli to erythromycin because of its presumed resistance to the
antibiotic.
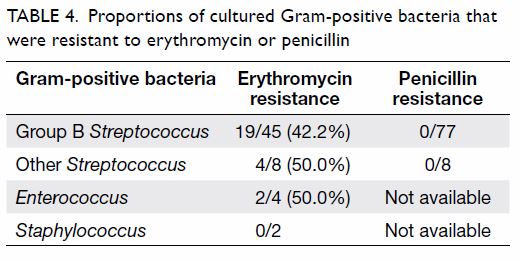
Table 4. Proportions of cultured Gram-positive bacteria that were resistant to erythromycin or penicillin
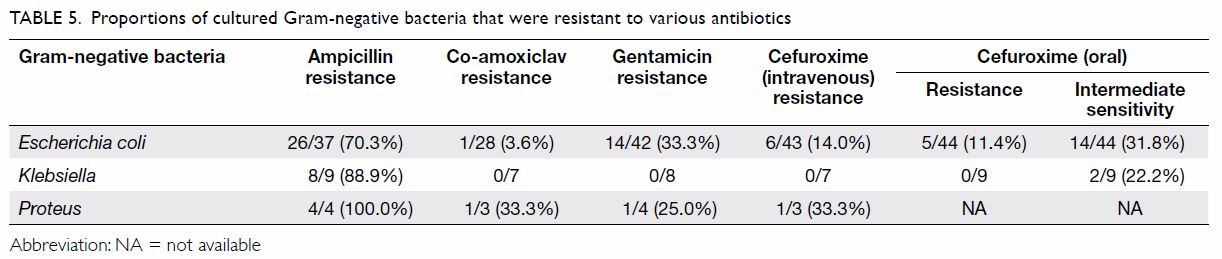
Table 5. Proportions of cultured Gram-negative bacteria that were resistant to various antibiotics
Discussion
The incidence of PPROM was 2.63% in our cohort,
which was consistent with prior reports in the literature.1 The identified risk factors for PPROM included advanced
maternal age, primiparity, and multiple pregnancies. Our cohort showed
that women with PPROM had greater incidences of preterm deliveries, lower
birthweight babies, and neonatal death, confirming a relationship between
PPROM and major neonatal morbidity and mortality.
Roles of Gram-positive and Gram-negative bacteria in
neonatal sepsis
A Korean study compared the incidences of
early-onset neonatal sepsis in cases of PPROM between two periods
(1996-2004 and 2005-2012) and found that the incidences of early-onset
neonatal sepsis due to Gram-positive bacteria were similar (1.5% vs 1.6%,
P=1.0) between the two periods, while the incidences of early-onset
neonatal sepsis due to Gram-negative bacteria were significantly different
(0.6% vs 2.7%, P=0.04).10 In our
cohort, the incidence of early-onset neonatal sepsis due to Gram-positive
bacteria was 3.1% (17/553), while the incidence of early-onset neonatal
sepsis due to Gram-negative bacteria was 2.9% (16/553). An Israeli study
investigated patients with preterm delivery (<37 weeks of gestation)
who had maternal fever, chorioamnionitis, or PPROM; the results showed
that early-onset neonatal sepsis was caused by E coli in 80% of
patients (12/15), whereas it was not caused by GBS in any patients.9 In our cohort, the incidences of early-onset neonatal
sepsis caused by GBS and E coli were both 2.0% (11/553). However,
the presence of E coli in maternal, placental, or neonatal
specimens was significantly associated with the development of early-onset
neonatal sepsis (P=0.004); this relationship was not observed with respect
to GBS (P=0.39). This was likely because of the prophylactic erythromycin
that was administered when patients were diagnosed with PPROM and the
benzyl penicillin administered when these patients were in labour; these
antibiotics were able to partially control GBS, but were generally unable
to control E coli. Therefore, it is important to administer an
antibiotic that can control both Gram-positive and Gram-negative bacteria
in PPROM patients.
Insufficient control of Escherichia coli by
ampicillin and erythromycin
There have been very few studies regarding
colonisation of female genital tracts by E coli, especially among
pregnant patients. In an analysis of 514 patients with female genital
tract infections during 2016 and 2017, 17.7% of the infections were found
to be caused by E coli; its rate of resistance to ampicillin was
67% (61/91).12 A large study
regarding the resistance of E coli in urinary tract infections
(n=42 033) from 1999 to 2009 found that its rate of resistance to
ampicillin was 58.3%.13 Such data
were consistent with our findings that 70.3% of E coli isolates
were resistant to ampicillin. With the exception of a meta-analysis in
Ethiopia that showed 52.9% of E coli isolates were resistant to
erythromycin,14 very few studies
in the literature have investigated the extent of E coli
resistance to erythromycin. It is generally believed that E coli
isolates are intrinsically resistant to low-level macrolide antibiotics
due to plasmid-mediated resistance; this includes a high rate of
resistance to erythromycin.15
Therefore, erythromycin is rarely used to treat E coli infection,
and most laboratories, including our centre, do not routinely perform
erythromycin sensitivity testing for E coli. However, most
international guidelines5 6 7 8 currently recommend the use of erythromycin, with or
without ampicillin, in PPROM patients. Based on the findings in our study,
this antibiotic regimen does not provide adequate control of E coli,
as it was most frequently identified as the cause of early-onset neonatal
sepsis.
Insufficient control of Group B Streptococcus
by erythromycin
Group B Streptococcus was detected in 14.6%
of maternal, placental, and neonatal specimens in our cohort; similarly,
in a study published in 2014, Yeung et al2
reported a GBS maternal carrier rate of 12.5% in PPROM patients. They
found that the rate of resistance to erythromycin was 65% among GBS
isolates, and that the incidence of neonatal GBS infection was
significantly lower in patients who received penicillin than in those who
received erythromycin (0.0% vs 36.4%; P=0.012). In addition, Yeung et al2 suggested that, instead of
erythromycin, ampicillin or amoxicillin should be administered to PPROM
patients who are active GBS carriers or whose GBS status is unknown.
Although our cohort demonstrated a lower rate of resistance (42.2%) of GBS
to erythromycin, we agree that the administration of erythromycin alone is
insufficient to control GBS. In addition, our findings demonstrated that
approximately half of the other Gram-positive bacterial isolates,
including Enterococcus and other Streptococcus bacteria,
were resistant to erythromycin; thus, the overall number of Gram-positive
bacterial isolates controlled by erythromycin could be as low as 42.4%
(25/59).
Potential use of other antibiotics and clinical
implications
Escherichia coli was found to have a low
rate of resistance to co-amoxiclav (3.6%); GBS was also expected to be
sensitive to co-amoxiclav because none of the GBS isolates were resistant
to penicillin in our cohort. However, the ORACLE 1 trial found that the
use of co-amoxiclav in PPROM patients was significantly associated with an
increased incidence of neonatal necrotising enterocolitis, compared with
the use of other antibiotics (1.8% vs 0.7%, P=0.0005).1 Most international guidelines discourage the use of
co-amoxiclav because of this finding.5
6 7
8 A Cochrane systematic review in
2013 assessed 22 randomised controlled trials regarding the use of
prophylactic antibiotics in PPROM; only three small trials had compared
the incidence of neonatal necrotising enterocolitis between placebo and
other penicillins that were not co-amoxiclav.3
Two trials investigated the use of mezlocillin (n=47 and n=40), whereas
the other investigated the use of piperacillin (n=37); none found an
increased incidence of neonatal necrotising enterocolitis.16 17 18 Mezlocillin is no longer available in the market as
it has been replaced by other penicillins with better bacterial coverage
such as piperacillin and ticarcillin. Piperacillin is typically reserved
for more severe infections that are resistant to cephalosporin; thus, it
is seldom prescribed as first-line treatment. Therefore, piperacillin may
not be suitable for use as antibiotic prophylaxis in asymptomatic PPROM
patients without evidence of acute chorioamnionitis. In our cohort, E
coli had a 14.0% of rate of resistance to intravenous cefuroxime,
and Klebsiella showed no resistance; thus, intravenous cefuroxime
could be appropriate for controlling both Gram-positive and Gram-negative
bacteria. Thus far, there have been no studies regarding the use of
cefuroxime in patients with PPROM. A large study regarding antibiotic
resistance rates of E coli isolates in urinary tract infections
(n=42 033), from 1999 to 2009, found that the rate of resistance to
cefuroxime was 3.7%.13 Finally,
one third (33.3%) of E coli isolates were resistant to gentamicin
in our cohort. A threshold of 20% has been suggested as the degree of
resistance at which an antibiotic should no longer be used empirically.19 Because of the resistance of E
coli to gentamicin and its potential side-effects in terms of
ototoxicity and nephrotoxicity, gentamicin is not recommended as a routine
prophylactic antibiotic in PPROM.
A study in Korea published in 2016 proposed the use
of a combination of ceftriaxone, clarithromycin, and metronidazole in
PPROM patients, and this new regimen was shown to more frequently
eradicate intra-amniotic inflammation or infection, as well as to more
frequently prevent secondary intra-amniotic inflammation or infection,
compared with an antibiotic regimen which included ampicillin and/or
cephalosporin.20 In our cohort,
only 1.8% of maternal, placental, or neonatal specimens demonstrated
growth of anaerobes, and these were not associated with early-onset
neonatal sepsis. Therefore, the use of metronidazole may not be essential
in PPROM patients. In the current recommendations from a variety of
international guidelines, erythromycin remains the most commonly used
macrolide with an established safety profile in perinatal use, relative to
other next-generation macrolides, such as clarithromycin. Therefore, we
recommend continued usage of erythromycin in PPROM patients, rather than
clarithromycin. However, Gram-positive and Gram-negative bacteria were
found in a total of 29.1% (161/553) patients with PPROM in our cohort.
Based on the presumption that all Gram-negative bacterial isolates were
resistant to erythromycin, the use of erythromycin alone as a
broad-spectrum antibiotic regimen was insufficient for control of
Gram-positive and Gram-negative bacteria in 67.7% (109/161) of these
culture-positive patients, or 19.7% (109/553) of all patients with PPROM
in our cohort. Therefore, additional antibiotics are needed to achieve
better control of GBS and Gram-negative bacteria, particularly E coli.
Co-amoxiclav is not recommended because it is associated with an increased
risk of neonatal necrotising enterocolitis. Based on our findings, we
propose the addition of intravenous cefuroxime. Ceftriaxone, a
third-generation cephalosporin, is presumed to be equally effective, or to
be more effective than cefuroxime, in controlling Gram-negative bacteria.
However, because of the risk of generating drug resistance in other
bacteria, such as Enterobacter,21
22 third-generation cephalosporins
may not be suitable for use in empirical antibiotic prophylaxis in
asymptomatic PPROM patients without evidence of acute chorioamnionitis.
Oral cefuroxime is more convenient to prescribe
than intravenous cefuroxime in PPROM patients. However, Gram-negative
bacteria were more sensitive to intravenous cefuroxime than oral
cefuroxime in our cohort: 31.8% of E coli and 22.2% of Klebsiella
only showed intermediate sensitivity to oral cefuroxime. Therefore, we
recommend the administration of a 1-week course of intravenous cefuroxime
in PPROM patients, combined with 10 days of oral erythromycin.
Furthermore, the efficacy of a combined regimen, such as 3 days of
intravenous cefuroxime followed by 4 days of oral cefuroxime, together
with oral erythromycin, needs additional analysis to determine whether
they are comparable in PPROM patients.
Limitations of this study
There were some limitations in our study. First,
our hospital laboratory did not perform sensitivity testing of
Gram-negative bacteria (including E coli) to erythromycin, because
of its assumed resistance. Second, our hospital laboratory did not perform
sensitivity testing of all isolated pathogens; instead, it performed
testing of pathogens with significant growth in culture, and such testing
was limited to the most commonly used antibiotics. Therefore, the full
spectrum of sensitivity of identified pathogens to various possible
antibiotics could not be fully established from the available data.
Because of our departmental guidelines for prescribing intrapartum benzyl
penicillin for patients with preterm labour, the clinical outcomes
observed in our cohort—particularly with regard to early-onset neonatal
sepsis—could have been influenced by the combined use of erythromycin and
intrapartum benzyl penicillin, rather than by the effect of erythromycin
alone.
Conclusion
Use of erythromycin with or without ampicillin was
insufficient to control Gram-positive and Gram-negative bacterial growth
in patients with PPROM. Based on the increase in Gram-negative bacteria
and the association of these bacteria with the development of early-onset
neonatal sepsis, intravenous cefuroxime (a second-generation
cephalosporin) is proposed for use as antibiotic prophylaxis, in
combination with erythromycin. Further studies regarding the use of
erythromycin combined with intravenous cefuroxime in PPROM patients are
suggested to investigate the efficacies of these antibiotics for
preventing early-onset neonatal sepsis, and to explore their side-effects,
such as the development of neonatal necrotising enterocolitis.
Author contributions
All authors had full access to the data,
contributed to the study, approved the final version for publication, and
take responsibility for its accuracy and integrity.
Concept or design of the study: CW Kong.
Acquisition of data: YY Li.
Analysis or interpretation of data: All authors.
Drafting of the article: YY Li, CW Kong.
Critical revision for important intellectual content: WWK To.
Acquisition of data: YY Li.
Analysis or interpretation of data: All authors.
Drafting of the article: YY Li, CW Kong.
Critical revision for important intellectual content: WWK To.
Conflicts of interest
All authors have disclosed no conflicts of
interest.
Funding/support
This research received no specific grant from any
funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
Ethics approval for this study was granted by the
Kowloon Central/Kowloon East Research Ethics Committee
(KC/KE18-0190/ER-1). As this study was a retrospective review, the need
for individual patient consent was waived by the research ethics
committee.
References
1. Kenyon SL, Taylor DJ, Tarnow-Mordi W;
ORACLE Collaborative Group. Broad-spectrum antibiotics for preterm,
prelabour rupture of fetal membranes: the ORACLE I randomised trial.
ORACLE Collaborative Group. Lancet 2001;357:979-88. Crossref
2. Yeung SW, Sahota DS, Leung TY.
Comparison of the effect of penicillins versus erythromycin in preventing
neonatal group B Streptococcus infection in active carriers
following preterm prelabor rupture of membranes. Taiwan J Obstet Gynecol
2014;53:210-4. Crossref
3. Kenyon S, Boulvain M, Neilson JP.
Antibiotics for preterm rupture of membranes. Cochrane Database Syst Rev
2013;(12):CD001058. Crossref
4. Mercer BM, Miodovnik M, Thurnau GR, et
al. Antibiotic therapy for reduction of infant morbidity after preterm
premature rupture of the membranes. A randomized controlled trial.
National Institute of Child Health and Human Development Maternal-Fetal
Medicine Units Network. JAMA 1997;278:989-95. Crossref
5. National Institute for Health and Care
Excellence. Preterm labour and birth. NICE guideline (NG25). Available
from:
https://www.nice.org.uk/guidance/ng25/resources/preterm-labour-and-birth-pdf-1837333576645.
Accessed 2 May 2019. Crossref
6. Committee on Practice
Bulletins—Obstetrics. ACOG Practice Bulletin No. 188: Prelabor rupture of
membranes. Obstet Gynecol 2018;131:e1-14. Crossref
7. Yudin MH, van Schalkwyk J, Van Eyk N.
No. 233—Antibiotic therapy in preterm premature rupture of the membranes.
J Obstet Gynaecol Can 2017;39:e207-12. Crossref
8. The Royal Australian and New Zealand
College of Obstetricians and Gynaecologists. Prophylactic antibiotics in
obstetrics and gynaecology. Available from:
https://www.ranzcog.edu.au/RANZCOG_SITE/media/RANZCOG-MEDIA/Women%27s%20Health/Statement%20and%20guidelines/Clinical%20-%20General/Prophylactic-antibiotics-in-obstetrics-and-gynaecology-(C-Gen-17)-Review-July-2016.pdf?ext=.pdf.
Accessed 2 May 2019.
9. Wolf MF, Miron D, Peleg D, et al.
Reconsidering the current preterm premature rupture of membranes
antibiotic prophylactic protocol. Am J Perinatol 2015;32:1247-50. Crossref
10. Jeong H, Han SJ, Yoo HN, et al.
Comparison of changes in etiologic microorganisms causing early onset
neonatal sepsis between preterm labor and preterm premature rupture of
membranes. J Matern Fetal Neonatal Med 2015;28:1923-8. Crossref
11. von Elm E, Altman DG, Egger M, et al.
The Strengthening the Reporting of Observational Studies in Epidemiology
(STROBE) statement: guidelines for reporting observational studies.
Epidemiology 2007;18:800-4. Crossref
12. Kim YA, Lee K, Chung JE. Risk factors
and molecular features of sequence type (ST) 131
extended-spectrum-β-lactamase-producing Escherichia coli in
community-onset female genital tract infections. BMC Infect Dis
2018;18:250. Crossref
13. Cullen IM, Manecksha RP, McCullagh E,
et al. The changing pattern of antimicrobial resistance within 42,033 Escherichia
coli isolates from nosocomial, community and urology
patient-specific urinary tract infections, Dublin, 1999-2009. BJU Int
2012;109:1198-206. Crossref
14. Tuem KB, Gebre AK, Atey TM, Bitew H,
Yimer EM, Berhe DF. Drug resistance patterns of Escherichia coli
in Ethiopia: a meta-analysis. Biomed Res Int 2018;2018:4536905. Crossref
15. Andremont A, Gerbaud G, Courvalin P.
Plasmid-mediated high-level resistance to erythromycin in Escherichia
coli. Antimicrob Agents Chemother 1986;29:515-8. Crossref
16. August Fuhr N, Becker C, van Baalen A,
Bauer K, Hopp H. Antibiotic therapy for preterm premature rupture of
membranes—results of a multicenter study. J Perinat Med 2006;34:203-6. Crossref
17. Johnston MM, Sanchez-Ramos L, Vaughn
AJ, Todd MW, Benrubi GI. Antibiotic therapy in preterm premature rupture
of membranes: a randomized, prospective, double-blind trial. Am J Obstet
Gynecol 1990;163:743-7. Crossref
18. Lockwood CJ, Costigan K, Ghidini A, et
al. Double-blind; placebo-controlled trial of piperacillin prophylaxis in
preterm membrane rupture. Am J Obstet Gynecol 1993;169:970-6. Crossref
19. Gupta K. Addressing antibiotic
resistance. Am J Med 2002;113 Suppl 1A:29S-34S. Crossref
20. Lee J, Romero R, Kim SM, Chaemsaithong
P, Yoon BH. A new antibiotic regimen treats and prevents intra-amniotic
inflammation/infection in patients with preterm PROM. J Matern Fetal
Neonatal Med 2016;29:2727-37.
21. Muller A, Lopez-Lozano JM, Bertrand X,
Talon D. Relationship between ceftriaxone use and resistance to
third-generation cephalosporins among clinical strains of Enterobacter
cloacae. J Antimicrob Chemother 2004;54:173-7. Crossref
22. Fung-Tomc JC, Gradelski E, Huczko E,
Dougherty TJ, Kessler RE, Bonner DP. Differences in the resistant variants
of Enterobacter cloacae selected by extended-spectrum
cephalosporins. Antimicrob Agents Chemother 1996;40:1289-93. Crossref