Hong Kong Med J 2025 Apr;31(2):119–29 | Epub 7 Apr 2025
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
ORIGINAL ARTICLE
Mask-wearing intention after the removal of the
mandatory mask-wearing requirement in Hong
Kong: application of the protection motivation
theory and the theory of planned behaviour
Tommy KC Ng, MSc1; Ben YF Fong, MPH, FHKAM (Community Medicine)1; Vincent TS Law, DBA, PMgr2; Pimtong Tavitiyaman, PhD3; WK Chiu, PhD1
1 Division of Science, Engineering and Health Studies, College of
Professional and Continuing Education, Hong Kong Polytechnic
University, Hong Kong SAR, China
2 Division of Social Sciences, Humanities and Design, College of
Professional and Continuing Education, Hong Kong Polytechnic
University, Hong Kong SAR, China
3 Division of Business and Hospitality Management, College of
Professional and Continuing Education, Hong Kong Polytechnic
University, Hong Kong SAR, China
Corresponding author: Mr Tommy KC Ng (tommy.ng@cpce-polyu.edu.hk)
 Full paper in PDF
Full paper in PDF
Abstract
Introduction: The mandatory mask-wearing
requirement, which had been in place for nearly
1000 days in Hong Kong, was lifted on 1 March
2023. Little is known about the intention to continue
wearing a mask after the removal of the mandate in
the city. This study aimed to examine predictors of
mask-wearing intention after the mandate was lifted,
using the protection motivation theory (PMT) and
the theory of planned behaviour (TPB).
Methods: A conceptual model was developed to
depict the relationships between the constructs of
PMT and TPB in predicting continued mask-wearing
intention after the removal of the mandate. A cross-sectional
study was conducted using an online
questionnaire from 8 to 20 March 2023. Partial least
squares structural equation modelling was utilised
to examine relationships between the constructs.
Results: In total, 483 responses were included
in the data analysis. Perceived severity (β=0.089;
P=0.017), perceived self-efficacy (β=0.253; P<0.001),
subjective norms (β=0.289; P<0.001), and attitude
(β=0.325; P<0.001) had significant positive effects
on the intention to continue wearing a mask. In
contrast, the perceived reward of maladaptive
behaviours had a significant negative effect on mask-wearing
intention (β=-0.071; P=0.012). Perceived
vulnerability, perceived response efficacy, perceived response cost, and perceived behavioural control
were not significantly associated with mask-wearing
intention.
Conclusion: The findings indicate that attitude
towards continued mask-wearing was the strongest
predictor of mask-wearing intention, followed
by subjective norms and perceived self-efficacy.
Insights from this study may inform public health
policymaking regarding mask-wearing practices in
future health crises.
New knowledge added by this study
- More than half of the respondents (53.6%) consistently wore a mask after the mandatory mask-wearing requirement had been lifted in Hong Kong.
- Attitude towards continued mask-wearing was the strongest predictor of mask-wearing intention, followed by subjective norms and perceived self-efficacy.
- A high frequency of mask-wearing was observed after the mandatory mask-wearing requirement had been lifted. The progress of Hong Kong citizens in returning to pre-pandemic norms requires further evaluation.
- The positive attitude towards mask-wearing among Hong Kong citizens suggests that they are prepared for future health crises.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic
has had extensive global social and health impacts.
It triggered an international health and economic
crisis that has profoundly altered people’s lives,
perceptions, and behaviours. As of 13 March 2025, about 778 million confirmed cases of COVID-19
had caused around 7.1 million deaths worldwide.1
Various levels of non-pharmaceutical interventions,
including frequent handwashing, mask-wearing,
and social distancing, were implemented in most
countries.2 These interventions played important roles in reducing community transmission of
COVID-19.3 However, the stringent measures also
led to negative consequences, such as economic
slowdown, disrupted education, and increased social
isolation and psychological stress.4 5 Many countries
lifted non-pharmaceutical interventions while the
number of cases was still increasing. In England,
all COVID-19–related restrictions were lifted on
22 February 2022 under the ‘Living with COVID’
strategy,6 although the number of cases increased
in subsequent months. Australia, Singapore, and
Hong Kong adopted a ‘Zero-COVID’ strategy.7 In
Australia, all mandatory mask-wearing requirements
on public transport were lifted in mid-September
2022.8 Singapore also lifted such requirements on 9 February 2023.9 Hong Kong, a leading international
business and financial centre, finally lifted all
mandatory mask-wearing requirements on 1
March 2023,10 nearly 1000 days after the start of
the pandemic in 2020. Since then, the city has been
transitioning towards the post–COVID-19 era.
During the COVID-19 pandemic, many
governments mandated mask-wearing in public
areas. Mask-wearing behaviour was largely a
response to legal restrictions and requirements.
Obedience, as a form of social influence, played a
role in mask adherence; individuals sought to avoid
social punishment, including fines or imprisonment.
Additionally, normative social influence emerged
as a means of curbing the spread of COVID-19. A positive correlation was observed between social
norms regarding mask-wearing and mask uptake,
such that individuals were more likely to wear a mask
if their friends and relatives did so.11 Furthermore,
individuals’ beliefs about engaging in the right
behaviour were associated with their behavioural
intentions. Personal norms regarding mask-wearing
were significantly associated with mask-wearing
intention.12 In the post–COVID-19 era, individuals
may continue mask-wearing even after governments
have lifted mandatory requirements, potentially
due to self-motivation for health protection. This
study aimed to identify predictors of mask-wearing
intentions and practices after the mandatory mask-wearing
requirement had been lifted in Hong Kong by
integrating the protection motivation theory (PMT)
with the theory of planned behaviour (TPB). This
integration provides a comprehensive framework for
evaluating mask-wearing intentions by examining
key factors influencing health behaviours, including
perceived severity, perceived vulnerability, attitudes,
and subjective norms. This approach may offer
a nuanced understanding of predictors of mask-wearing
intentions after the mandatory mask-wearing
requirement had been lifted.
Protection motivation theory
Protection motivation theory has been widely
used as a framework for predicting the adoption of
health-protective behaviours.13 This theory assumes
that the adoption of protective behaviour against
health threats depends on personal motivation for
self-protection. Rooted in expectancy-value theory,
PMT explains the social and cognitive processes
underlying protective behaviours. The theory is
based on the premise that the decision to counteract
a health threat is determined by threat and coping
appraisal processes.14 According to PMT, two
primary processes—threat appraisal and coping
appraisal—determine behavioural intention. Threat
appraisal consists of three components: perceived
vulnerability, perceived severity, and the perceived
reward of maladaptive behaviours. Perceived
vulnerability refers to an individual’s assessment
of the likelihood of experiencing a health threat or
developing a health condition. Perceived severity
concerns the perceived seriousness of potential
consequences associated with the condition.
Therefore, perceptions of COVID-19 severity and
vulnerability to disease would significantly predict
adherence to protective measures.15 Perceived reward
of maladaptive behaviours refers to beliefs regarding
the benefits associated with engaging in risky
behaviours. Patients with COVID-19 may experience
long COVID symptoms, including increased fatigue,
depressive symptoms, and reduced mental acuity.16
In this context, individuals may continue wearing
masks due to concerns about long-COVID severity. Thus, perceived vulnerability and perceived severity
are expected to be positively associated with the
intention to continue wearing a mask in the post–COVID-19 era, whereas the perceived reward of
maladaptive behaviours is expected to be negatively
associated with this behaviour. Three hypotheses
were proposed in relation to these elements (H1 to
H3 in the online supplementary Table).
Coping appraisal comprises perceived response
efficacy, perceived self-efficacy, and perceived
response cost. Perceived response efficacy refers
to belief in the effectiveness of the recommended
behaviour with respect to mitigating or preventing
potential harm.17 Perceived self-efficacy denotes
an individual’s confidence in overcoming barriers
to implementing the recommended behaviour.18
Perceived response cost refers to perceived costs
associated with the behaviour. Perceived response
efficacy has been positively associated with social
distancing behaviours, a non-pharmaceutical
intervention for COVID-19, among Hong Kong
adults.19 Three hypotheses were derived in relation to these elements (H4 to H6 in the online supplementary Table).
Theory of planned behaviour
The TPB is a well-established model for explaining
health-related behavioural intentions, which
are influenced by subjective norms (perceived
expectations from significant others regarding
the behaviour), attitude (personal feelings and
beliefs about the behaviour), and perceived
behavioural control (perceived ability to perform
the behaviour). Individuals with a more positive
attitude towards non-pharmaceutical interventions
exhibit a greater intention to implement such
interventions.20 Similarly, subjective norms and
perceived behavioural control have demonstrated
positive associations with the intention to adopt
interventions against COVID-19.20 Five hypotheses
were formulated in relation to these elements (H7 to
H11 in the online supplementary Table).
Integration of protection motivation theory
and theory of planned behaviour
The integration of PMT and TPB has been utilised
to predict behavioural intention in various
research contexts, such as adherence to COVID-19
behavioural guidelines,21 behavioural intention
towards COVID-19 booster vaccination,22 and
factors affecting preventive behaviours during
the COVID-19 pandemic.23 In this study, the
attitude component of TPB was used to assess an
individual’s attitude towards continuing to wear a
mask. Attitudes may be influenced by an individual’s
protection motivation. A meta-analysis identified
perceived importance, perceived benefits, perceived
effectiveness, and perceived barriers to preventive behaviour as key attitudinal factors influencing
such behaviour.24 Therefore, a conceptual model
was developed to illustrate relationships between
the constructs of PMT and TPB in predicting
continued mask-wearing after the announcement
that all mandatory mask-wearing requirements had
been lifted. Fourteen hypotheses were formulated in
relation to these elements (H12 to H25 in the online supplementary Table).
Methods
Participant recruitment
This cross-sectional study was conducted using
an online questionnaire between 8 and 20 March
2023. Participants were recruited through a non-probability
snowball sampling method that had been
used in a previous study.3 The target sample size was
determined based on the requirement that it should
be 10 times the maximum number of measurement
items associated with a single construct in the partial
least squares path model.25 In this study, 37 items
measured ten constructs, resulting in a target sample
size of 370 (10 × 37). The online questionnaire was
distributed via email and WhatsApp, a widely
used social media platform in Hong Kong. Using
the researchers’ personal social networks, eligible
individuals of various ages and educational
backgrounds were invited to participate. They were
also encouraged to share the questionnaire link with
suitable colleagues and friends. Additionally, the
researchers contacted the heads of local community
colleges to seek collaboration and support. Upon
receiving approval from directors or presidents, the
researchers sent the online questionnaire to those
leaders for recruitment of eligible participants.
Individuals were included in this study if they
were Hong Kong residents aged ≥18 years and
had access to the internet via a smartphone or
computer. Participants read a statement on the
survey’s background, anonymity, and participation
agreement before providing consent. To prevent
duplicate submissions, the prefix and first three
digits of the Hong Kong Identity Card were collected
and later removed prior to data analysis.
Measures within the questionnaire
The questionnaire, consisting of four sections,
was designed to assess perceived vulnerability,
perceived severity, perceived reward of maladaptive
behaviours, perceived response efficacy, perceived
self-efficacy, perceived response cost, attitude,
perceived behavioural control, subjective norms,
and intention to continue wearing a mask after the
mandatory mask-wearing requirement had been
lifted. The first section included two questions
focused on mask-wearing frequency after the
mandatory requirement had been lifted and on verification of Hong Kong residency. The second
section examined respondents’ adoption of health-protective
behaviours, based on PMT.26 27 The third
section measured variables related to respondents’
intention to continue wearing a mask, based on
TPB.3 27 All items in the second and third sections
were assessed using a five-point Likert scale
(1=strongly disagree to 5=strongly agree). The final
section collected demographic information, such as
age, gender, education level, economic status, and
self-reported health status, through close-ended
questions.
Data analysis
Partial least squares structural equation modelling
was utilised to examine the conceptual framework
in this study. The SmartPLS 3.0 statistical software
(SmartPLS GmbH, Bönningstedt, Germany) was
used to assess both the reflective measurement
model and the structural model. Study reliability
and validity were evaluated by assessing internal
consistency and convergent validity in the reflective
measurement model.25 Convergent validity was
considered acceptable if the outer loadings of the
measurement items exceeded 0.5 and the average
variance extracted for each construct was >0.5.25 28
Internal reliability was evaluated using composite
reliability, which was recommended to exceed 0.708,
and Cronbach’s alpha, which should be >0.6.25 Path
coefficients were assessed within the structural
model. A P value <0.05 was considered significant.
Results
Participant characteristics
In total, 483 valid responses were included in the
data analysis. Table 1 presents the participants’
demographic characteristics. The largest proportion
of respondents belonged to the 18-25 age-group
(28.2%), followed by the 56-65 (18.4%), the 66-75
(13.7%), and the 36-45 (13.0%) age-groups. The
mean age was 43.56 years. Among the participants,
269 (55.7%) were men and 214 (44.3%) were
women. Most respondents (59.0%) had attained a
degree-level education or higher; more than two-fifths
of respondents were employed. Additionally,
approximately half of the respondents (46.6%) rated
their health status as good. More than half of the
respondents (53.6%) reported always wearing a mask
after the mandatory mask-wearing requirement
had been lifted. The median number of COVID-19
vaccine doses received was three (interquartile
range=1).
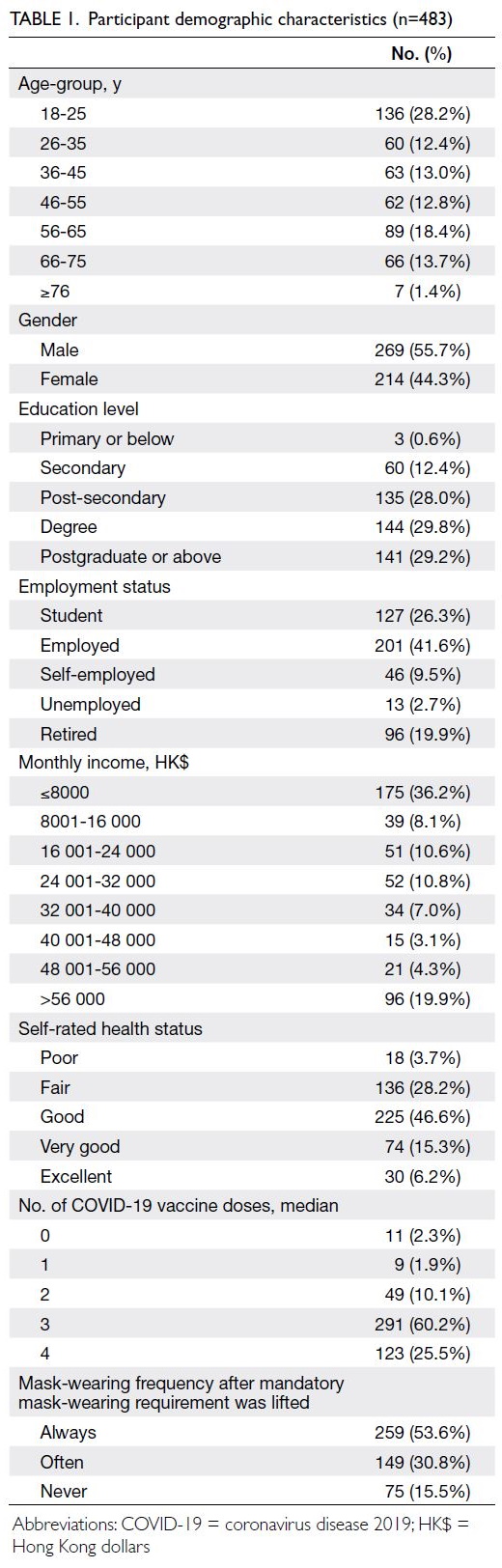
Table 1. Participant demographic characteristics (n=483)
Measurement model
Table 2 presents the model reliability. Loadings >0.7
indicate a satisfactory level of item reliability.25 29 The
outer loadings of all items exceeded 0.7, except for one item related to perceived behavioural control;
consequently, this item was removed. Internal
consistency reliability was considered satisfactory
because composite reliability and Cronbach’s
alpha exceeded the threshold value of 0.7. The
average variance extracted for all constructs was
>0.5, suggesting good convergent validity after the
removal of five items: one item each from perceived
severity, perceived response efficacy, perceived
self-efficacy, attitude, and behavioural intention.
The variance inflation factor for each item was <5,
indicating no critical levels of collinearity. Table 3
depicts the results of the assessment of discriminant validity. Given the adequacy of indicator reliability,
internal consistency reliability, convergent validity,
and discriminant validity, evaluation of the structural
model could proceed.29
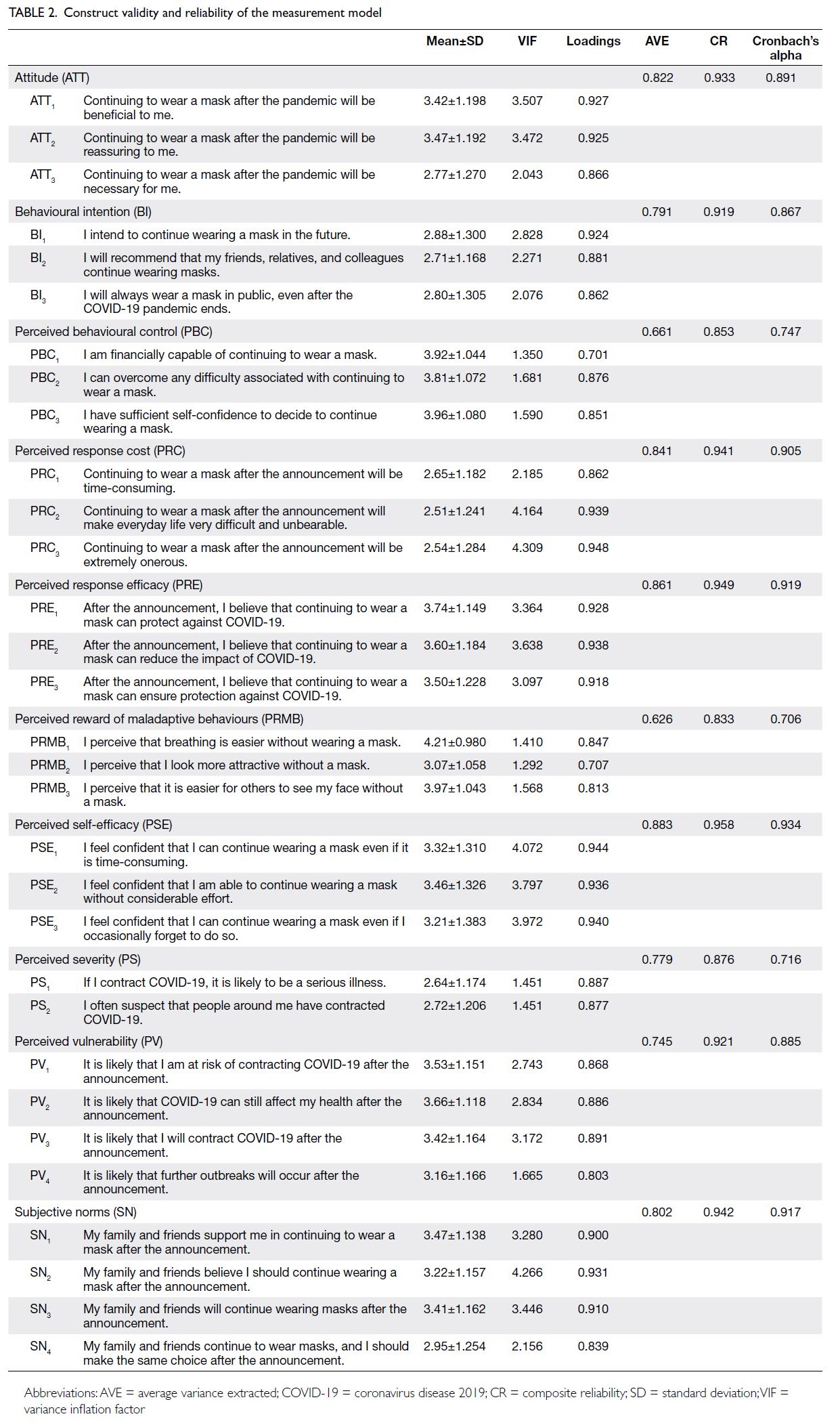
Table 2. Construct validity and reliability of the measurement model
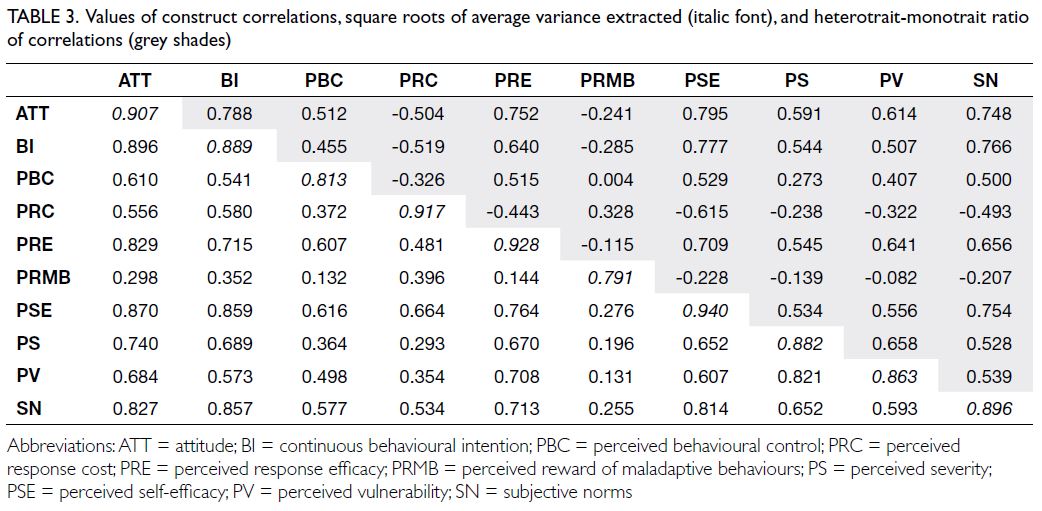
Table 3. Values of construct correlations, square roots of average variance extracted (italic font), and heterotrait-monotrait ratio of correlations (grey shades)
Structural model
Table 4 displays the results of direct effects in the
structural model. Of the 17 hypotheses, 10 were
supported based on the results generated through
a bootstrapping procedure with 5000 resamples.
Four constructs—perceived severity, perceived
self-efficacy, subjective norms, and attitude—had
significant positive effects on the intention to continue wearing a mask. In contrast, perceived
reward of maladaptive behaviours had a significant
negative effect on mask-wearing intention.
Consequently, hypotheses H2, H3, H5, H7, and H8
were supported. However, perceived vulnerability,
perceived response efficacy, perceived response
cost, and perceived behavioural control were
not significantly associated with the intention to
continue wearing a mask. Thus, hypotheses H1, H4,
H6, and H9 were not supported.
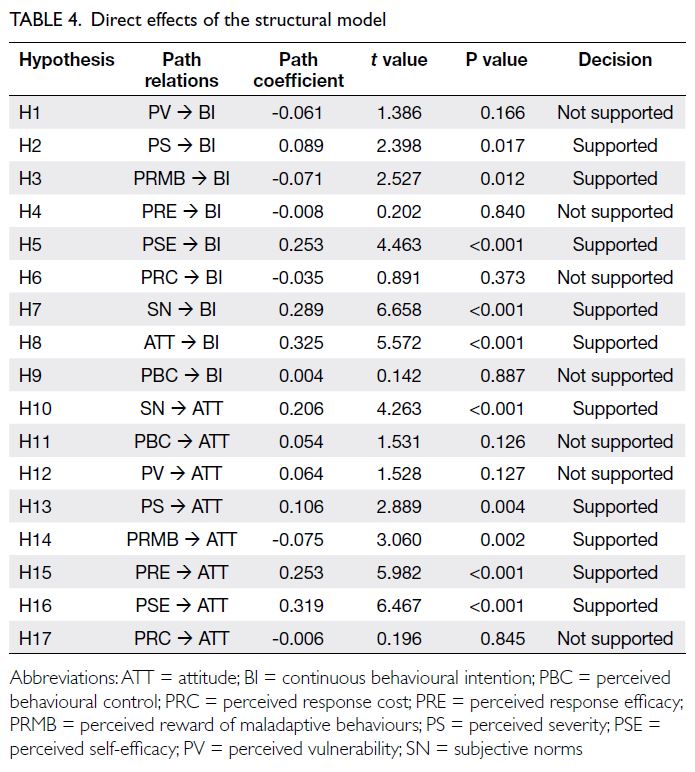
Table 4. Direct effects of the structural model
Furthermore, subjective norms, perceived
severity, perceived response efficacy, and perceived
self-efficacy had significant positive effects on
attitude, whereas perceived reward of maladaptive
behaviours had a significant negative effect on
attitude. Therefore, hypotheses H10, H13, H14, H15,
and H16 were supported. However, no significant
relationships were observed between perceived
behavioural control and attitude, perceived
vulnerability and attitude, or perceived response
cost and attitude. These findings did not support
hypotheses H11, H12, and H17 (Table 4). The results
of the structural model are depicted in the Figure.
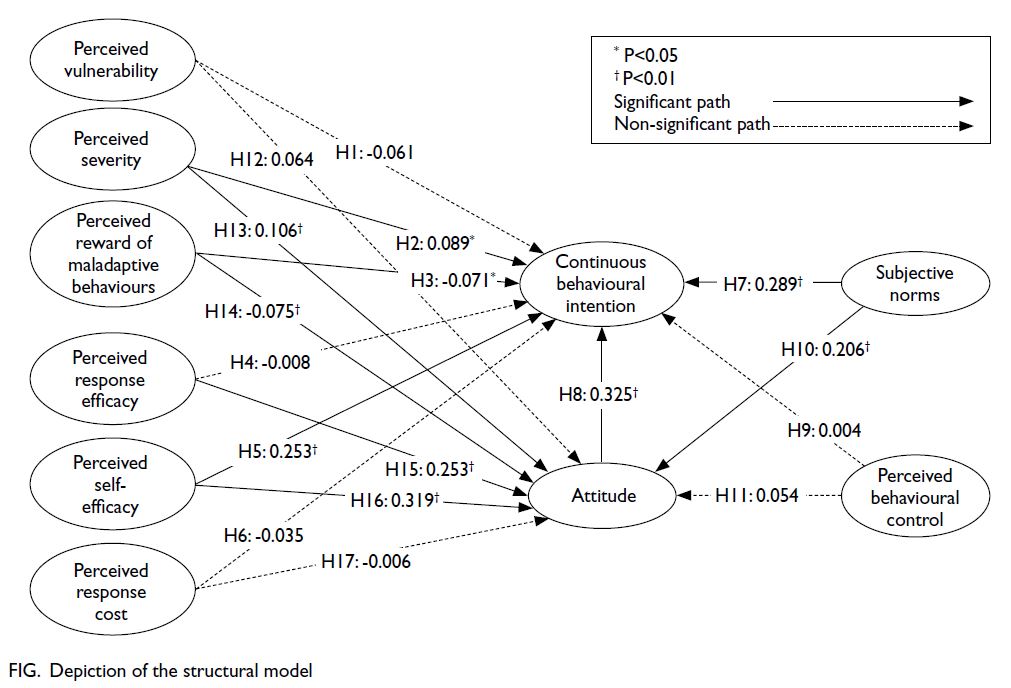
Figure. Depiction of the structural model
Table 5 shows the results of the mediation
model. Attitude had a partial mediating effect on
the relationships of perceived self-efficacy, perceived
reward of maladaptive behaviours, subjective
norms, and perceived severity with the intention to continue wearing a mask. These results partially
supported hypotheses H19, H20, H21, and H22.
Additionally, attitude had a full mediating effect on
the relationship between perceived response efficacy
and the intention to continue wearing a mask,
supporting hypothesis H24. However, no mediating
effect of attitude was observed in the relationships
of perceived response cost, perceived vulnerability,
and perceived behavioural control with continuous
behavioural intention. These results did not support
hypotheses H18, H23, and H25.
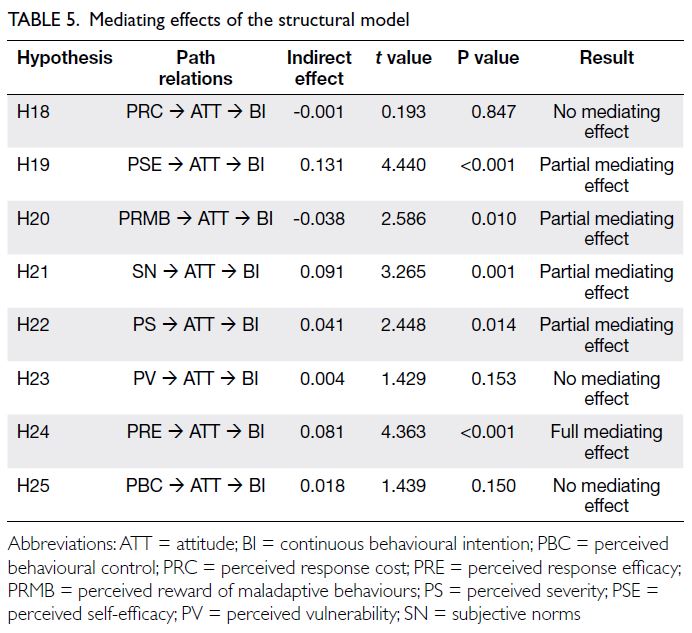
Table 5. Mediating effects of the structural model
Discussion
Most respondents continued wearing masks during
the 3 weeks after the mandatory mask-wearing
requirement had been lifted. Perceived severity,
perceived self-efficacy, subjective norms, and
attitude were positively associated with the intention
to continue wearing a mask, whereas the perceived
reward of maladaptive behaviours was negatively
associated with this intention. Perceived severity
suggests that individuals were concerned about the
consequences of contracting COVID-19. Given that
COVID-19 had influenced daily life and behaviour
for 3 years, it is understandable that perceived
severity remained a motivator for continued mask-wearing
as a protective measure. Furthermore, some
individuals may have experienced anxiety and sought
to minimise the risk of infection. Thus, the pandemic
itself may have outweighed their desire to return to
pre-pandemic norms.30 Additionally, perceived self-efficacy
indicates that individuals with confidence in their ability to wear a mask effectively were more
likely to continue doing so. Personal protective
measures can reduce the risk of infectious diseases31;
mask-wearing is considered a feasible and acceptable
method for preventing and reducing the spread of
influenza-like illnesses.32 During the COVID-19
pandemic, some studies showed that perceived
severity and perceived self-efficacy were significantly
associated with intentions to comply with COVID-19
preventive behaviours.17 33 34 Individuals perceived
that contracting COVID-19 posed a serious threat,
whereas mask-wearing remained a feasible and
effective strategy for preventing transmission, even
after the mandatory mask-wearing requirement had
been lifted.
Notably, the perceived reward of maladaptive
behaviours had a significant negative effect on the
intention to continue wearing a mask. This finding
suggests that individuals who perceived benefits
from not wearing a mask were less likely to express
an intention to continue mask-wearing. The decision
not to wear a mask may be attributed to various
factors, including concerns about social judgement,
the inconveniences associated with preventive
measures, and daily hassles.35 36 The prolonged
COVID-19 pandemic led to pandemic fatigue, which
may have contributed to a perception among some
individuals that the pandemic had ended once the
mandatory mask-wearing requirement was lifted,
thereby reducing their motivation to continue
wearing a mask.
Attitudes and subjective norms had significant
positive effects on the intention to continue wearing
a mask. This observation indicates that individuals
who held a favourable attitude towards mask-wearing
and perceived social pressure or influence
from others to wear a mask were more likely to
express an intention to continue this practice.
Attitudes and subjective norms were previously
identified as predictors of mask-wearing intention
during the COVID-19 pandemic.3 Before the
pandemic, the local population in Hong Kong
exhibited a positive attitude towards mask-wearing.
For example, patients and caregivers in outpatient
settings generally wore face masks; protecting
others was a primary motivation for this approach.37
Individuals with a positive attitude towards mask-wearing
may have been influenced by government-led
promotion of preventive behaviours since the
severe acute respiratory syndrome epidemic in 2003,
which caused mask-wearing to become a social
norm within the community.38 The present findings
indicate that higher levels of perceived self-efficacy,
perceived reward of maladaptive behaviours,
subjective norms, and perceived severity not only
directly increased the intention to wear a mask but
also influenced individuals’ attitudes, leading to
an increased intention to continue mask-wearing. These results provide empirical evidence supporting
the role of attitude as a mediator in the intention to
continue wearing a mask. Thus, the relationships
among perceived self-efficacy, perceived reward of
maladaptive behaviours, subjective norms, perceived
severity, and the intention to continue mask-wearing
can also be explained by individuals’ attitudes.
In the present study, perceived vulnerability did
not directly predict the intention to continue wearing
a mask. A study also showed no significant association
between perceived vulnerability and the adoption
of preventive behaviours.39 A possible explanation
is that the prolonged COVID-19 pandemic led
individuals to consider themselves less vulnerable
compared with early stages of the pandemic. The
removal of government restrictions may have further
reinforced the perception of reduced vulnerability to
COVID-19.40 Additionally, the results of this study
did not demonstrate a statistically significant direct
effect between perceived response efficacy and the
intention to continue wearing a mask. However,
a mediating role for attitude was identified in this
relationship, indicating that perceived response
efficacy influenced attitude, which then determined
the intention to wear a mask.
Implications
This study highlights the importance of understanding
the predictors of mask-wearing intention after the
mandatory mask-wearing requirement was lifted.
A high frequency of mask-wearing was observed
after the removal of the requirement. This finding
has implications for future research regarding the
long-term effects of habitual mask use and its impact
on public health. From a practical perspective, the
findings indicate that attitude towards continued
mask-wearing was the strongest predictor of mask-wearing
intention, suggesting that citizens are
prepared for future health crises. Policymakers
can utilise these insights to develop guidelines
encouraging mask use during influenza seasons.
Limitations
This study had certain limitations. First, the
sampling method relied on non-probability snowball
sampling, which may affect the representativeness
of the sample. Second, participation was limited to
individuals with access to email and social media,
leading to overrepresentation of younger and more
educated individuals. Younger participants may
consider themselves less likely to experience severe
health consequences if they contract COVID-19.
Consequently, the findings may not be generalisable
to the entire population.
Conclusion
To our knowledge, this is one of the first studies to use an online questionnaire to identify the
predictors of mask-wearing intention after the
mandatory mask-wearing requirement in Hong
Kong was lifted in March 2023. Attitude towards
continued mask-wearing, subjective norms, and
perceived self-efficacy exhibited strong positive
effects on the intention to continue wearing a
mask. Regarding research implications, this study
provides new insights into the evaluation of Hong
Kong citizens’ transition to a post-pandemic era.
The high frequency of mask-wearing observed may
be attributed to concerns about COVID-19 and
the establishment of mask-wearing as an accepted
and habitual behaviour within the local population.
Furthermore, the findings suggest that Hong Kong
citizens are well prepared for future health crises,
such as severe acute respiratory syndrome and
additional COVID-19 outbreaks. The positive
attitude towards mask-wearing reflects recognition
of its feasibility and effectiveness as a durable non-pharmaceutical
public health intervention to reduce
airborne disease transmission.
Author contributions
Concept or design: TKC Ng, BYF Fong.
Acquisition of data: All authors.
Analysis or interpretation of data: TKC Ng, BYF Fong.
Drafting of the manuscript: TKC Ng, BYF Fong.
Critical revision of the manuscript for important intellectual content: All authors.
Acquisition of data: All authors.
Analysis or interpretation of data: TKC Ng, BYF Fong.
Drafting of the manuscript: TKC Ng, BYF Fong.
Critical revision of the manuscript for important intellectual content: All authors.
All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Conflicts of interest
All authors have disclosed no conflicts of interest.
Funding/support
This research received no specific grant from any funding
agency in the public, commercial, or not-for-profit sectors.
Ethics approval
This research was approved by the Research Committee
of the College of Professional and Continuing Education of
Hong Kong Polytechnic University, Hong Kong (Ref No.:
RC/ETH/H/133). Informed consent was obtained from all
participants prior to the study and for the publication of this
research.
Supplementary material
The supplementary material was provided by the authors and
some information may not have been peer reviewed. Accepted
supplementary material will be published as submitted by the
authors, without any editing or formatting. Any opinions
or recommendations discussed are solely those of the
author(s) and are not endorsed by the Hong Kong Academy
of Medicine and the Hong Kong Medical Association.
The Hong Kong Academy of Medicine and the Hong Kong
Medical Association disclaim all liability and responsibility arising from any reliance placed on the content.
References
1. World Health Organization. WHO COVID-19 Dashboard.
Available from: https://covid19.who.int/. Accessed 13 Mar 2025.
2. Lison A, Banholzer N, Sharma M, et al. Effectiveness
assessment of non-pharmaceutical interventions: lessons
learned from the COVID-19 pandemic. Lancet Public
Health 2023;8:e311-7. Crossref
3. Duan Y, Shang B, Liang W, et al. Predicting hand washing,
mask wearing and social distancing behaviors among older
adults during the COVID-19 pandemic: an integrated
social cognition model. BMC Geriatr 2022;22:91. Crossref
4. Diallo I, Ndejjo R, Leye MM, et al. Unintended consequences
of implementing non-pharmaceutical interventions for the
COVID-19 response in Africa: experiences from DRC,
Nigeria, Senegal, and Uganda. Global Health 2023;19:36. Crossref
5. ÓhAiseadha C, Quinn GA, Connolly R, et al. Unintended
consequences of COVID-19 non-pharmaceutical
interventions (NPIs) for population health and health
inequalities. Int J Environ Res Public Health 2023;20:5223. Crossref
6. Limb M. COVID-19: scientists and medics warn that
it is too soon to lift all restrictions in England. BMJ
2022;376:o469. Crossref
7. Zhan Z, Li J, Cheng ZJ. Zero-COVID strategy: what’s next?
Int J Health Policy Manag 2023;12:6757. Crossref
8. Dunstan J. Victoria to ease COVID-19 mask mandate
on public transport from 11:59pm Thursday. ABC News
[newspaper on the Internet]. 2022 Sep 21. Available from:
https://www.abc.net.au/news/2022-09-21/victoria-mask-mandate-ends-trains-trams-buses-transport/101460606. Accessed 7 Jul 2024.
9. Lin C. Singapore relaxes COVID travel curbs, mask rules
further. Reuters [newspaper on the Internet]. 2023 Feb
9. Available from: https://www.reuters.com/world/asia-pacific/singapore-relaxes-covid-travel-curbs-mask-rules-further-2023-02-09/. Accessed 7 Jul 2024.
10. Hong Kong SAR Government. Government lifts all
mandatory mask-wearing requirements [press release].
2023 Feb 28. Available from: https://www.info.gov.hk/gia/general/202302/28/P2023022800677.htm. Accessed 13 Mar 2025.
11. Barceló J, Sheen GC. Voluntary adoption of social welfare-enhancing
behavior: mask-wearing in Spain during the
COVID-19 outbreak. PloS One 2020;15:e0242764. Crossref
12. Lipsey NP, Losee JE. Social influences on mask-wearing
intentions during the COVID-19 pandemic. Soc Pers
Psychol Compass 2023;17:e12817. Crossref
13. Ezati Rad R, Mohseni S, Kamalzadeh Takhti H, et al.
Application of the protection motivation theory for
predicting COVID-19 preventive behaviors in Hormozgan,
Iran: a cross-sectional study. BMC Public Health
2021;21:466. Crossref
14. Fischer-Preßler D, Bonaretti D, Fischbach K. A protection-motivation
perspective to explain intention to use and
continue to use mobile warning systems. Bus Inf Syst Eng
2022;64:167-82. Crossref
15. González-Castro JL, Ubillos-Landa S, Puente-Martínez A,
Gracia-Leiva M. Perceived vulnerability and severity predict adherence to COVID-19 protection measures:
the mediating role of instrumental coping. Front Psychol
2021;12:674032. Crossref
16. Bierbauer W, Lüscher J, Scholz U. Illness perceptions in
long-COVID: a cross-sectional analysis in adults. Cogent
Psychol 2022;9:2105007. Crossref
17. Lahiri A, Jha SS, Chakraborty A, Dobe M, Dey A. Role
of threat and coping appraisal in protection motivation
for adoption of preventive behavior during COVID-19
pandemic. Front Public Health 2021;9:678566. Crossref
18. Bandura A. The growing centrality of self-regulation in
health promotion and disease prevention. Eur Health
Psychol 2005;7:11-2.
19. Yu Y, Lau JT, Lau MM. Competing or interactive effect
between perceived response efficacy of governmental
social distancing behaviors and personal freedom on
social distancing behaviors in the Chinese adult general
population in Hong Kong. Int J Health Policy Manag
2022;11:498-507. Crossref
20. Ohnmacht T, Hüsser AP, Thao VT. Pointers to interventions
for promoting COVID-19 protective measures in tourism:
a modelling approach using domain-specific risk-taking
scale, theory of planned behaviour, and health belief model.
Front Psychol 2022;13:940090. Crossref
21. Nudelman G. Predicting adherence to COVID-19
behavioural guidelines: a comparison of protection
motivation theory and the theory of planned behaviour.
Psychol Health 2024;39:1689-705. Crossref
22. Zhou M, Liu L, Gu SY, et al. Behavioral intention and its
predictors toward COVID-19 booster vaccination among
Chinese parents: applying two behavioral theories. Int J
Environ Res Public Health 2022;19:7520. Crossref
23. Khaday S, Li KW, Dorloh H. Factors affecting preventive
behaviors for safety and health at work during the
COVID-19 pandemic among Thai construction workers.
Healthcare (Basel) 2023;11:426. Crossref
24. Liang W, Duan Y, Li F, et al. Psychosocial determinants of
hand hygiene, facemask wearing, and physical distancing
during the COVID-19 pandemic: a systematic review and
meta-analysis. Ann Behav Med 2022;56:1174-87. Crossref
25. Hair Jr JF, Hult GT, Ringle CM, Sarstedt M. A Primer on
Partial Least Squares Structural Equation Modeling (PLS-SEM).
Los Angeles [CA]: Sage Publications; 2021.
26. Youn SY, Lee JE, Ha-Brookshire J. Fashion consumers’
channel switching behavior during the COVID-19:
protection motivation theory in the extended planned
behavior framework. Cloth Text Res J 2021;39:139-56. Crossref
27. Zhang X, Liu S, Wang L, Zhang Y, Wang J. Mobile health
service adoption in China: integration of theory of planned
behavior, protection motivation theory and personal health
differences. Online Inf Rev 2020;44:1-23. Crossref
28. Ting MS, Goh YN, Isa SM. Determining consumer
purchase intentions toward counterfeit luxury goods in
Malaysia. Asia Pac Manage Rev 2016;21:219-30. Crossref
29. Sarstedt M, Ringle CM, Hair JF. Partial least squares
structural equation modeling. In: Homburg C, Klarmann
M, Vomberg AE, editors. Handbook of Market Research.
Switzerland: Springer International Publishing; 2021: 587-632. Crossref
30. Mo PK, Yu Y, Lau MM, Ling RH, Lau JT. Time to lift up
COVID-19 restrictions? Public support towards living
with the virus policy and associated factors among Hong
Kong general public. Int J Environ Res Public Health 2023;20:2989. Crossref
31. Masai AN, Akin L. Practice of COVID-19 preventive
measures and risk of acute respiratory infections: a
longitudinal study in students from 95 countries. Int J
Infect Dis 2021;113:168-74. Crossref
32. Polonsky JA, Bhatia S, Fraser K, et al. Feasibility,
acceptability, and effectiveness of non-pharmaceutical
interventions against infectious diseases among crisis-affected
populations: a scoping review. Infect Dis Poverty
2022;11:14. Crossref
33. Acar D, Kıcali ÜÖ. An integrated approach to COVID-19
preventive behaviour intentions: protection motivation
theory, information acquisition, and trust. Soc Work
Public Health 2022;37:419-34. Crossref
34. Kwok KO, Li KK, Chan HH, et al. Community responses
during early phase of COVID-19 epidemic, Hong Kong.
Emerg Infect Dis 2020;26:1575-9. Crossref
35. Lai DW, Jin J, Yan E, Lee VW. Predictors and moderators of
COVID-19 pandemic fatigue in Hong Kong. J Infect Public Health 2023;16:645-50. Crossref
36. Rieger MO. To wear or not to wear? Factors influencing
wearing face masks in Germany during the COVID-19
pandemic. Asian J Soc Health Behav 2020;3:50-4. Crossref
37. Ho HS. Use of face masks in a primary care outpatient
setting in Hong Kong: knowledge, attitudes and practices.
Public Health 2012;126:1001-6. Crossref
38. Mo PK, Lau JT. Illness representation on H1N1 influenza
and preventive behaviors in the Hong Kong general
population. J Health Psychol 2015;20:1523-33. Crossref
39. Zancu SA, Măirean C, Diaconu-Gherasim LR. The
longitudinal relation between time perspective and
preventive behaviors during the COVID-19 pandemic:
the mediating role of risk perception. Curr Psychol
2024;43:12981-9. Crossref
40. Stefanczyk MM, Rokosz M, Białek M. Changes in perceived
vulnerability to disease, resilience, and disgust sensitivity
during the pandemic: a longitudinal study. Curr Psychol
2024;43:23412-24. Crossref