Hong Kong Med J 2024 Jun;30(3):209–17 | Epub 21 May 2024
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
ORIGINAL ARTICLE
Healthy Eating Report Card for Pre-school Children in Hong Kong
Alison WL Wan, MSc; Kevin KH Chung, PhD; JB Li, MEd, PhD; Derwin KC Chan, MSc, PhD
Department of Early Childhood Education, The Education University of Hong Kong, Hong Kong SAR, China
Corresponding author: Dr Derwin KC Chan (derwin@eduhk.hk)
 Full paper in PDF
Full paper in PDF
Abstract
Introduction: This study aimed to develop the
Healthy Eating Report Card for Pre-school Children
in Hong Kong for evaluating the prevalence of healthy
eating behaviours and favourable family home food
environments (FHFEs) among pre-school children
in Hong Kong.
Methods: In this cross-sectional study, 538 parent-child
dyads from eight kindergartens in Hong Kong
were recruited. Parents or guardians completed a
questionnaire comprising Report Card items. The
Report Card included two indicators of Children’s
Eating Behaviours (ie, Children’s Dietary Patterns
and Children’s Mealtime Behaviours) and three
indicators of FHFEs (ie, Parental Food Choices and
Preparation, Avoidance of Unhealthy Foods, and
Family Mealtime Environments). Each indicator
and its specific items were assigned a letter grade
representing the percentage of participants
achieving the predefined benchmarks. The grades
were defined as A (≥80%, Excellent); B (60%-79%,
Good); C (40%-59%, Fair); D (20%-39%, Poor); and F
(<20%, Very poor). Plus (+) and minus (-) signs were
used to indicate the upper or lower 5% of each grade.
Results: Overall, Children’s Eating Behaviours were classified as Fair (average grade of ‘C’), whereas
FHFEs were classified as Good (average grade
of ‘B’). The sub-grades ranged from ‘C’ to ‘A-’, as
follows: Children’s Dietary Patterns, ‘C+’; Children’s
Mealtime Behaviours, ‘C’; Parental Food Choices and
Preparation, ‘C+’; Avoidance of Unhealthy Foods, ‘B’;
and Family Mealtime Environments, ‘A-’.
Conclusion: The findings highlight areas for
improvement in healthy eating among children.
The Healthy Eating Report Card could offer novel
insights into intervention tools that promote healthy
eating.
New knowledge added by this study
- Eating behaviours among pre-school children in Hong Kong were classified as Fair (average grade of ‘C’).
- Among those children, family home food environments (FHFEs) were classified as Good (average grade of ‘B’).
- There is considerable potential for improvement in children’s dietary patterns, children’s mealtime behaviours, and parental food choices and preparation.
- The Healthy Eating Report Card for Pre-school Children can be considered a useful tool for evaluating the prevalence of healthy eating behaviours and favourable FHFEs among pre-school children.
- The grades provided by the Report Card offer valuable guidance concerning how healthy eating behaviours and favourable FHFEs among pre-school children could be promoted at the family, school, and community levels.
Introduction
Unhealthy dietary patterns, generally characterised
by low dietary diversity, skipping breakfast, low
consumption of fruits and vegetables, and frequent
consumption of energy-dense/nutrient-poor foods
and sugar-sweetened beverages, are common
among children worldwide.1 2 It is particularly
important for young children to adopt healthy
dietary patterns because eating habits and food
preferences in childhood can influence dietary
patterns in adulthood.3 Similar to children in other regions, Hong Kong children have a high prevalence
of unhealthy dietary patterns.4 A cross-sectional
survey evaluating infant and young child feeding
practices in Hong Kong identified numerous dietary
problems, including dietary imbalance (eg, high
protein but low fibre intake), overdependence on the
use of formula milk, inadequate intake of vegetables
and fruits, and unhealthy snacking and sugary
beverage habits.5 A previous study revealed a need for dietary improvement among Hong Kong pre-school
children.6 Key recommendations included a balanced diet, better nutritional adequacy, and
greater independence during mealtimes (ie, self-feeding).6 Indeed, inappropriate behaviours during
mealtimes, such as lack of self-feeding, food refusal,
picky eating, and prolonged meals, are common
in young children.7 8 Children with inappropriate
mealtime behaviours may be susceptible to
insufficient nutrient and/or energy intake.9 However,
there is limited information available regarding the
mealtime behaviours of typically developing pre-school
children in Hong Kong.
Family home food environments (FHFEs), ie,
parental food choices and preparation, avoidance of
unhealthy foods, and family mealtime environments,
have strong associations with children’s dietary habits
and body weight.10 11 12 Parental use of nutrition labels
to make healthier food choices has been linked to a
lower probability of overweight or obesity in their
children.13 Similarly, children with limited access
to unhealthy foods are reportedly more likely to
maintain a normal body weight.14 A review focusing
on the effects of family and social environment on
children’s dietary patterns found that a structured
mealtime environment—namely, regular meals with
family members and screen-free mealtimes—was
associated with healthy food consumption patterns
in children.15 In summary, children’s mealtime
behaviours and FHFEs are important for healthy
eating among young children. Thus far, no studies
have provided an overview of eating behaviours and FHFEs among pre-school children in Hong Kong.
The use of a report card at the country-/region-level can provide a valuable overview of
the prevalence of health behaviours through a
conventional letter grading system (ranging from
A+ to F).16 This framework has been used to evaluate
various health-related behaviours (eg, physical
activity,17 18 19 sedentary behaviour,17 18 19 smoking
behaviour,20 and dietary patterns20 21 22) in children and
youth. The findings of such report cards offer insights
concerning the extent to which health behaviours
are adopted in specific communities and provide
targeted recommendations for health behaviours
at the individual or public level.16 23 Moreover, the
publication of these report cards can facilitate health
promotion awareness and catalyse policy changes
that motivate individuals to commit to health
behaviours.16 19 24 Thus far, only one published report
card (the Healthy Active Kids South Africa [HAKSA]
Report Card) has revealed dietary patterns among
children and youth.21 However, the HAKSA Report
Card only covered the intake of fruits, vegetables, and
unhealthy snacks; other essential aspects of healthy
eating (eg, daily breakfast consumption, dietary
variety, mealtime behaviours, and FHFEs) were
not considered. Additionally, because the evidence
underlying the grading criteria for various aspects of
healthy eating was not explicitly stated, the findings
of the HAKSA Report Card might not provide useful
benchmarks concerning how well individuals adhere
to healthy eating standards or recommendations
adopted by health authorities. Therefore, we aimed
to address the aforementioned research gaps
through a cross-sectional study that developed the
Healthy Eating Report Card for Pre-school Children
in Hong Kong, using a grading scale and evidence-based
benchmarks to assess the current prevalence
of healthy eating behaviours and favourable FHFEs
among pre-school children in Hong Kong.
Our Report Card assesses various indicators of
Children’s Eating Behaviours (ie, Children’s Dietary
Patterns and Children’s Mealtime Behaviours) and
FHFEs (ie, Parental Food Choices and Preparation,
Avoidance of Unhealthy Foods, and Family Mealtime
Environments). Each indicator and its specific items
are assigned letter grades based on predefined
benchmarks, revealing how well pre-school children
in Hong Kong meet the recommendations and
standards established by the government and
published literature concerning pre-school children’s
healthy eating behaviours and FHFEs (Tables 125 26 27 28 29 30 31
and 223). The findings may enhance the understanding
of eating behaviours and FHFEs among pre-school
children in Hong Kong. Additionally, the Healthy
Eating Report Card established in our study will
be useful for future studies examining healthy
eating among young children in other countries or
regions.
Methods
Participants
We recruited 538 Hong Kong parent-child dyads
from eight local kindergartens in three main regions
of Hong Kong (29.55% of children from the New
Territories, 62.64% of children from Kowloon, and
7.81% of children from Hong Kong Island). The
children were aged between 2 and 6 years with a
mean age of 4.10 years (standard deviation=0.92);
49.63% of the children were boys. Of the children,
33.77%, 29.46%, and 36.77% were in grades K1, K2,
and K3, respectively. Respondents were mainly
mothers (85.63%), followed by fathers (13.25%) and
other legal guardians (1.12%). The mean respondent
age was 36.62 years (standard deviation=5.84).
Procedures
This cross-sectional study examined the prevalence
of healthy eating behaviours and favourable FHFEs
among Hong Kong pre-school children in October
2021. We sent invitation letters to 89 randomly
selected local kindergartens across 18 districts
in Hong Kong (excluding international schools
and special needs schools). Eight kindergartens
agreed to participate in this study and distribute
our questionnaire to eligible parents. The inclusion
criteria required participants to: (1) be Chinese parents or guardians; (2) have at least one child in
grades K1 to K3; and (3) have sufficient Chinese
reading ability to complete the questionnaire. Schools
and parents were both asked to provide written
informed consent. Parents completed a parent-reported
questionnaire (comprising the Healthy
Eating Report Card items) about their children’s
eating behaviours and FHFEs, which typically
required 15 minutes to complete. Respondents
received a HK$50 supermarket voucher as a token of
appreciation for their participation.
Report Card questionnaire
The design of our Healthy Eating Report Card was
based on the conceptual framework established by
the Report Card on Physical Activity for Children
and Youth, which offers a comprehensive grading
framework and benchmarks to evaluate health
behaviours.16 17 18 19 20 21 22 23 The Global Matrix 3.0 Physical
Activity Report Card for Children and Youth has
been used in 49 countries to evaluate the prevalence
of physical activity behaviours among children and
youth.23 Using a similar assessment framework, our
Healthy Eating Report Card evaluated the prevalence
of healthy eating behaviours and favourable FHFEs
among Hong Kong pre-school children. The Healthy
Eating Report Card Questionnaire consisted of
21 items which were developed based on the healthy eating guidelines and recommendations
of the Department of Health of Hong Kong.25 26
The items were aligned with the five indicators of
our Report Card, including two Children’s Eating
Behaviours indicators (ie, Children’s Dietary
Patterns and Children’s Mealtime Behaviours) and
three FHFEs indicators (ie, Parental Food Choices
and Preparation, Avoidance of Unhealthy Foods,
and Family Mealtime Environments), to determine
whether the children adhered to healthy eating
behaviours and were involved in healthy FHFEs.
Participants responded to questionnaire items
using a 5-point Likert scale (ranging from ‘always’
to ‘never’), yes/no questions, open-ended questions,
and multiple-choice questions. The questionnaire is
provided in online supplementary Appendix 1.
Data analysis
Benchmarks for each indicator were established
in accordance with recommendations and
guidelines for healthy eating behaviours and
FHFEs from the Hong Kong SAR Government and
published literature.25 26 27 28 29 30 31 Based on the results of the
questionnaire, we used a benchmark framework
to determine the letter grade for each indicator
that reflected the percentage of participants who
met the predetermined benchmarks. A sub-grade
was also determined for each indicator item. The
questionnaire items and criteria of questionnaire
answers related to the benchmarks are displayed
in online supplementary Appendix 2.25 26 28 29 30 31 The
grading system for the Healthy Eating Report
Card was derived from the grading rubric of the
Global Matrix 3.0 Physical Activity Report Card
for Children and Youth, ie, A (≥80%, Excellent); B (60%-79%, Good); C (40%-59%, Fair); D (20%-39%,
Poor); and F (<20%, Very poor).23 Plus (+) and minus
(-) signs were used to show the upper or lower 5%
of each grade.23 The proposed benchmarks and the
grading scheme are shown in Tables 125 26 27 28 29 30 31 and 2,23
respectively.
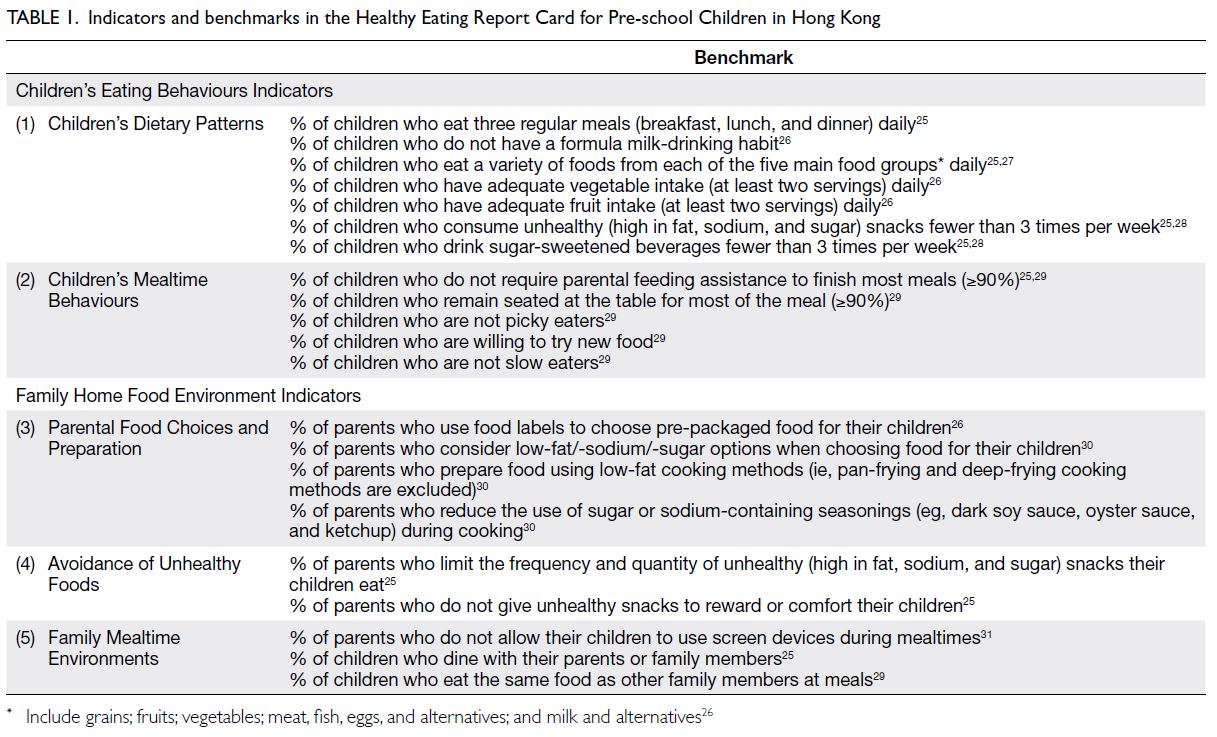
Table 1. Indicators and benchmarks in the Healthy Eating Report Card for Pre-school Children in Hong Kong

Table 2. Grading system of the Healthy Eating Report Card for Pre-school Children in Hong Kong
Due to the percentage calculation, responses
to 5-point Likert scale questions in the questionnaire
were converted to binary variables; responses of
‘sometimes’, ‘often’ and ‘always’ were categorised as
‘yes’, whereas responses of ‘never’ and ‘rarely’ were
categorised as ‘no’.32 All statistical analyses were
performed using SPSS software (Windows version
26.0; IBM Corp, Armonk [NY], United States).
Missing values ranged from 0.19% to 2.79% for
questionnaire items because of nonresponses to
some items. The descriptive statistics revealed valid
percentages for each indicator item, along with 95%
confidence intervals (CIs). The arithmetic mean
for each indicator was calculated by summing the
valid percentage for each item of the indicator, then
dividing that value by the number of corresponding
items. This arithmetic mean represents the average
percentage of participants who met predefined
benchmarks for that indicator.
Results
The letter grades of our Healthy Eating Report
Card are summarised in Table 3. The descriptive
statistics of the Report Card are displayed in online supplementary Appendix 3. The average grades of Children’s Eating Behaviours indicators and FHFEs
indicators were ‘C’ and ‘B’, respectively, showing
that the eating behaviours of Hong Kong pre-school
children were classified as Fair, whereas FHFEs were classified as Good (Table 3). On average, nearly half
of the pre-school children (52.88%; 95% CI=51.26%-54.50%) adhered to healthy eating behaviours,
whereas more than half of the parents (70.87%; 95%
CI=69.34%-72.40%) provided their children with
favourable FHFEs.
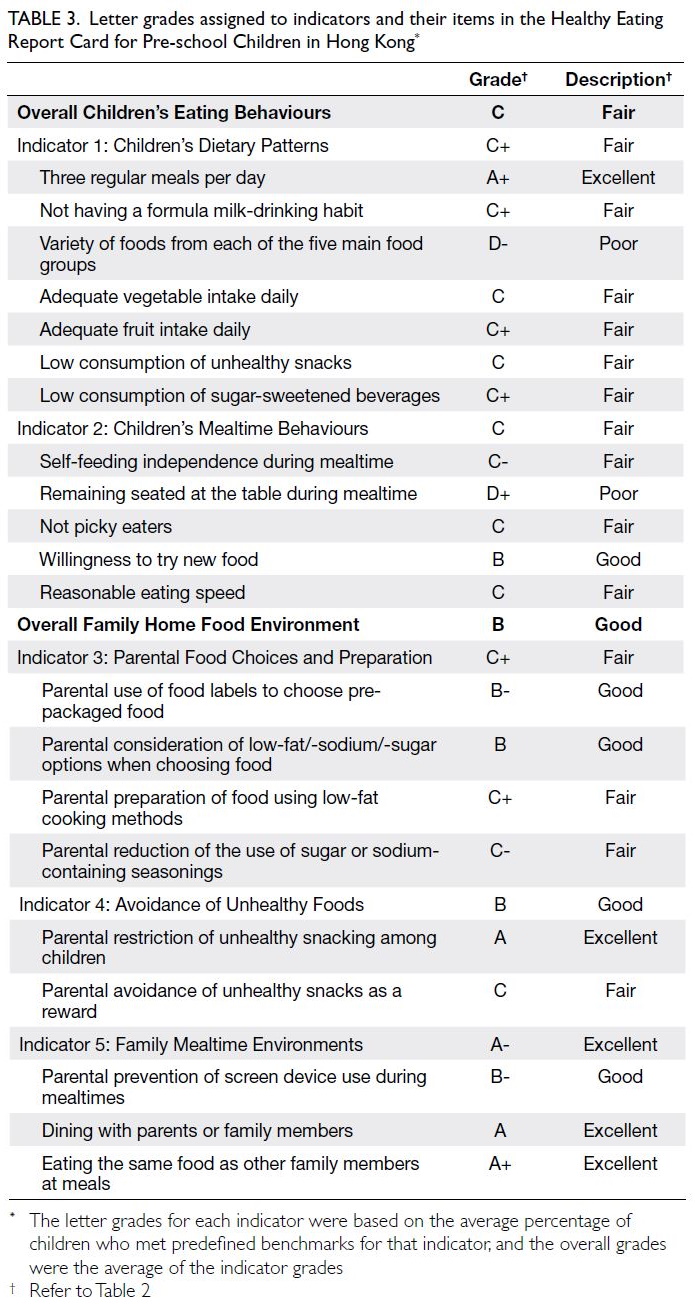
Table 3. Letter grades assigned to indicators and their items in the Healthy Eating Report Card for Pre-school Children in Hong Kong
Children’s Dietary Patterns
Nearly all children (97.58%) had three regular meals
daily. However, only 24.34% of the children ate a
variety of foods. Approximately half of the children
had adequate vegetable and fruit intakes (50.84%
and 58.40%, respectively). Moreover, 55.76% did not
have a formula milk-drinking habit. Additionally,
around half of the children had low consumption
of unhealthy snacks and sugary beverages (52.25%
and 58.87%, respectively) [online supplementary Appendix 3]. Overall, Children’s Dietary Patterns
was graded ‘C+’ (Fair), signifying that approximately
half of the children (55.37%; 95% CI=53.98%-56.75%)
adhered to healthy dietary patterns.
Children’s Mealtime Behaviours
Fewer than half of the children (43.02%) did not
require parental assistance to finish a meal. Only
38.32% of the children could remain seated during
mealtimes. Of the children, 49.15% and 67.98%
did not exhibit picky eating behaviours and were
willing to try new foods, respectively. Nearly half
of the children (49.35%) did not exhibit slow-eating
behaviours (online supplementary Appendix 3). Children’s Mealtime Behaviours was graded
‘C’ (Fair), showing that approximately half of the
children (49.92%; 95% CI=46.28%-55.07%) exhibited
desirable mealtime behaviours.
Parental Food Choices and Preparation
More than half of the parents (63.69%) used nutrition
labels. Similarly, more than half of the parents
(70.26%) considered low oil/salt/sugar food options
for their children. Approximately half of the parents
used low-fat cooking methods and reduced the use
of sugar- or salt-containing condiments (53.53%
and 43.58%, respectively) [online supplementary Appendix 3]. Parental Food Choices and Preparation
was graded ‘C+’ (Fair), revealing that approximately
half of the parents (57.88%; 95% CI=55.49%-60.28%)
made healthy food choices and prepared healthy
meals for their children.
Avoidance of Unhealthy Foods
Half of the parents (52.04%) did not reward their
children with unhealthy snacks or drinks. A
large majority of the parents (90.15%) limited the
frequency and quantity of unhealthy foods (online supplementary Appendix 3). Therefore, Avoidance
of Unhealthy Foods was graded ‘B’ (Good), signifying that more than half of the parents (71.10%; 95%
CI=68.66%-73.53%) controlled their children’s access
to unhealthy foods.
Family Mealtime Environments
A large majority of the children dined with their
parents or family members and ate the same food
as other family members (93.47% and 95.50%, respectively). More than half of the parents (61.08%)
did not allow their children to use screen devices
during mealtimes (online supplementary Appendix 3). Family Mealtime Environments was graded ‘A-’
(Excellent), showing that most children (83.46%;
95% CI=81.63%-85.29%) were involved in structured
family mealtime environments.
Discussion
This study aimed to develop the Healthy Eating
Report Card for Pre-school Children in Hong Kong,
which assessed the prevalence of healthy eating
behaviours and favourable FHFEs among pre-school
children in Hong Kong. We established evidence-based
benchmarks to guide the process of grading
Children’s Eating Behaviours indicators and FHFEs
indicators, then utilised letter grades to illustrate how
well children adhered to healthy eating behaviours.
Children’s Dietary Patterns and Children’s Mealtime
Behaviours were graded ‘C+’ and ‘C’, respectively,
signifying that eating behaviours in Hong Kong pre-school
children were Fair; the average overall grade
was ‘C’. Our findings indicate that approximately half
of the pre-school children in Hong Kong adhered to
healthy eating behaviours. Parental Food Choices
and Preparation, Avoidance of Unhealthy Foods,
and Family Mealtime Environments were graded
‘C+’, ‘B’, and ‘A-’, respectively, showing that FHFEs
were Good; the average overall grade was ‘B’. Our
results revealed that more than half of the pre-school
children in Hong Kong were involved in a
healthy home eating environment. Taken together,
these findings enhance the understanding of pre-school
children’s eating behaviours and FHFEs in
Hong Kong.
Comparison of Report Card findings with Hong Kong’s previous data
Our Report Card showed that the eating behaviours
of Hong Kong pre-school children were classified as
Fair; some unhealthy dietary patterns and undesirable
mealtime behaviours were prevalent because
nearly half of the children did not meet predefined
benchmarks for Children’s Eating Behaviours
indicators. Previous research33 concerning the
eating habits of Hong Kong pre-school children
showed that more than half of the surveyed children
(78.8%) had a habit of eating breakfast. Nevertheless,
fewer than half of the children achieved the
recommended daily intakes of vegetables (19.6%)
and fruits (47.3%), respectively.33 Some studies
identified a high prevalence of formula milk drinking
among Hong Kong pre-school–aged children, such
that 77% of 4-year-old children continue to drink
formula milk.5 34 Overdependence on formula milk
may reduce appetite in children and impede their
development of healthy eating habits.35 Lo et al33 found that, on average, children consumed high
energy-dense foods (eg, candy/chocolate, sweet
crackers, and sugary beverages) more than twice per
week; accordingly they suggested that such children
should minimise their consumption of these foods.
Additionally, an investigation regarding undesirable
mealtime behaviours among Hong Kong pre-school
children revealed that approximately 70% of the
children required >30 minutes to finish a meal;
these children often were unwilling to self-feed or
finish their meals.6 The present study are consistent
with previous research, indicating that there is
considerable potential for improvement in eating
behaviours among Hong Kong children.
Comparison of Report Card findings with
international data
As mentioned above, the HAKSA Report Card
assessed a few aspects of the dietary patterns of
South African children and youth aged 3 to 8 years
in 2018. Although using a grading rubric similar
to our Report Card, the HAKSA Report Card only
involved two indicators, namely Fruit and Vegetable
Intake (graded ‘D’) and Snacking, Sugar-Sweetened
Beverages, Dietary Sodium, and Fast Food Intake
(graded ‘F’).21 Our Report Card may provide better
coverage of healthy dietary patterns because it
included assessments of regular daily meals, food
variety, and formula milk-drinking habits, with a
particular focus on pre-school children aged 2 to 6
years. Despite the discrepancies between studies,
the healthy dietary patterns observed in our Report
Card were more favourable than patterns observed
in the HAKSA Report Card.21 This difference also
implies that standards for healthy eating behaviours
among children differ between South Africa and
Hong Kong. Future studies should develop a cross-ountry/region–level Report Card and establish
a global benchmark to comprehensively analyse
global variations in healthy eating, thereby raising
global awareness and stimulating global discussion
regarding the promotion of healthy eating.
Novel findings on family home food environments
Very little is known about FHFEs of children in
Hong Kong; therefore, the present study provides
initial information concerning parental food choices
and preparation, avoidance of unhealthy foods, and
family mealtime environments among Hong Kong
pre-school children. Based on our findings, the
FHFEs of the pre-school children in Hong Kong were
classified as Good. This result suggests that parents
in Hong Kong attempt to promote healthy diets by
limiting their children’s consumption of unhealthy
foods. A previous study revealed that Hong Kong
parents tended to adopt the ‘control over eating’ approach to feed their children, whereby parents
primarily determine the amounts of food that
children should eat, including unhealthy snacks.33
Moreover, parents often used food to reward or
comfort children.36 The indicator of Family Mealtime
Environments in our Report Card showed that most
pre-school children had a structured family mealtime
environment where they dined with their family and
shared the same food with their family members. This
finding may be attributed to the Chinese cultural
emphasis on shared meals with family members.37
Thus, the results of the present study are consistent
with previous research findings.
However, this high grade for Family Mealtime
Environments may have increased the average grade
for FHFEs indicators. Indeed, parents’ food choices,
purchases, and preparation directly influence
children’s home food environment and food
consumption.38 When we specifically focused on the
Parental Food Choices and Preparation indicator,
the grade decreased to Fair (letter grade of ‘C+’),
signifying that only half of the parents complied
with healthy eating practices for their children,
such as the use of nutrition labels and adoption of
healthy cooking methods. Thus, it is important to
promote healthy eating at home, which will facilitate
healthy eating behaviours among children. A pilot
FHFE intervention of the Healthy Home Offerings
via the Mealtime Environment Plus programme,
which provided parents and children with nutrition
education and meal preparation training and
activities, successfully promoted a structured
mealtime environment at home and helped to
improve dietary intake patterns.39 40 Accordingly,
future studies might utilise nutrition education
interventions to improve the FHFEs of pre-school
children in Hong Kong.
Strengths and limitations
This study had some strengths. In particular, we
collected primary data to enhance the understanding
of eating behaviours and FHFEs among pre-school
children in Hong Kong. Moreover, to our knowledge,
this is the first use of a report card framework to
comprehensively evaluate the prevalence of healthy
eating behaviours among pre-school children.41 The
Report Card can serve as an effective awareness-raising
tool that provides novel insights concerning
the promotion of healthy eating behaviours, as well
as recommendations for healthy eating policies and
healthy food environments.23
However, this study also had several limitations.
First, its cross-sectional design precluded the
identification of changes in children’s eating
behaviours and FHFEs over time. Future studies could
perform longitudinal measurements of variables
in the Report Card to reveal changes or stability in
healthy eating behaviours among young children; such measurements could also determine whether
Report Card scores are predictive of health outcomes
in children. An individual-level Healthy Eating
Report Card should be developed in future studies
to examine the effectiveness of the Report Card on
parental intentions towards healthy eating, as well as
children’s healthy eating behaviours and favourable
FHFEs. Second, although the items of the Healthy
Eating Report Card Questionnaire were developed
based on the guidelines and recommendations of the
Hong Kong SAR Government,25 26 the development
of the questionnaire did not include evaluations of
its content validity and psychometric properties.
Future studies should examine the psychometric
properties and other validity aspects of the Report
Card questionnaire (eg, factorial validity, convergent
validity, and discriminant validity).42 Third, the
study relied on parent-reported questionnaires of
children’s eating behaviours and FHFEs, which may
be susceptible to response biases, social desirability
bias, and general response tendencies.43 44 Validation
studies comparing parent-reported questionnaires
with more objective measures of children’s food
intake and observational assessments of mealtime
behaviours could be conducted in the future. Finally,
the current Report Card does not reflect several
components of children’s eating behaviours (eg, the
frequency of dining out and the variety of vegetable
and fruit consumption) and FHFEs (eg, parental
feeding practices and accessibility of healthy food
at home). Future studies should investigate whether
these components could be included within the
Healthy Eating Report Card to provide a more
holistic assessment of healthy eating among children.
Conclusion
This study developed the Healthy Eating Report
Card for Pre-school Children in Hong Kong to
reflect the prevalence of healthy eating behaviours
and favourable FHFEs among pre-school children in
Hong Kong. The Report Card revealed that Children’s
Eating Behaviours were classified as Fair (average
grade of ‘C’), whereas FHFEs were classified as Good
(average grade of ‘B’). There is considerable potential
for improvement in children’s eating behaviours (ie,
healthy dietary patterns and appropriate mealtime
behaviours) and FHFEs (particularly concerning
parental healthy food choices and preparation). We
believe that the Report Card can serve as a useful
tool for evaluating the prevalence of healthy eating
behaviours and favourable FHFEs in young children;
it could offer novel insights into strategies for
promotion of healthy eating in pre-school setting.
Author contributions
Concept or design: All authors.
Acquisition of data: AWL Wan, DKC Chan.
Analysis or interpretation of data: AWL Wan, DKC Chan.
Drafting of the manuscript: AWL Wan, DKC Chan.
Critical revision of the manuscript for important intellectual content: All authors.
Acquisition of data: AWL Wan, DKC Chan.
Analysis or interpretation of data: AWL Wan, DKC Chan.
Drafting of the manuscript: AWL Wan, DKC Chan.
Critical revision of the manuscript for important intellectual content: All authors.
All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Conflicts of interest
All authors have disclosed no conflicts of interest.
Acknowledgement
The authors thank Ms Kiko KH Leung, Ms Roni MY Chiu, and
Ms Tracy CW Tang from the Department of Early Childhood
Education of The Education University of Hong Kong for their
assistance in preparing study materials and collecting data.
The authors also thank the eight participating kindergartens
for aiding in the distribution and collection of questionnaires
from parents.
Funding/support
This research was funded by the Research Impact Cluster
Fund of the Department of Early Childhood Education,
Faculty of Education and Human Development, The
Education University of Hong Kong, through an award to
the corresponding author. The funder had no role in study
design, data collection/analysis/interpretation or manuscript
preparation.
Ethics approval
The study protocol of this research was approved by the
Human Research Ethics Committee of The Education
University of Hong Kong (Ref No.: 2020-2021-0420). All
schools and parents provided written informed consent for
participation in this research and have also consented to the
publication of its findings.
Supplementary material
The supplementary material was provided by the authors and
may include some information that was not peer reviewed.
Accepted supplementary material will be published as
submitted by the authors, without any editing or formatting.
Any opinions or recommendations discussed are solely
those of the author(s) and are not endorsed by the Hong
Kong Academy of Medicine and the Hong Kong Medical
Association. The Hong Kong Academy of Medicine and the
Hong Kong Medical Association disclaim all liability and
responsibility arising from any reliance placed on the content.
References
1. World Health Organization. Healthy diet. 2020. Available
from: https://www.who.int/news-room/fact-sheets/detail/healthy-diet. Accessed 9 Jul 2022.
2. Kupka R, Siekmans K, Beal T. The diets of children:
overview of available data for children and adolescents.
Glob Food Sec 2020;27:100442. Crossref
3. Movassagh EZ, Baxter-Jones AD, Kontulainen S, Whiting SJ,
Vatanparast H. Tracking dietary patterns over 20 years
from childhood through adolescence into young adulthood: the Saskatchewan Pediatric Bone Mineral Accrual Study. Nutrients 2017;9:990.Crossref
4. Department of Health. Hong Kong SAR Government.
Diet, physical activity and health: Hong Kong situation.
2010. Available from: https://www.change4health.gov.hk/filemanager/common/image/strategic_framework/action_plan/action_plan_2_e.pdf . Accessed 5 Jul 2022.
5. Woo J, Chan R, Li L, Luk WY. A survey of infant and young
child feeding in Hong Kong: diet and nutrient intake. 2012.
Available from: https://www.fhs.gov.hk/english/reports/files/Diet_nutrientintake_executive%20summary_2504.pdf . Accessed 5 Jul 2022.
6. Yip PS, Chan VW, Lee QK, Lee HM. Diet quality and eating
behavioural patterns in preschool children in Hong Kong.
Asia Pac J Clin Nutr 2017;26:298-307. Crossref
7. Crist W, Napier-Phillips A. Mealtime behaviors of young
children: a comparison of normative and clinical data. J
Dev Behav Pediatr 2001;22:279-86. Crossref
8. Archer LA, Rosenbaum PL, Streiner DL. The children’s
eating behavior inventory: reliability and validity results. J
Pediatr Psychol 1991;16:629-42. Crossref
9. Samuel TM, Musa-Veloso K, Ho M, Venditti C, Shahkhalili-Dulloo Y. A narrative review of childhood picky eating and its relationship to food intakes, nutritional status, and
growth. Nutrients 2018;10:1992. Crossref
10. Boswell N, Byrne R, Davies PS. Family food environment
factors associated with obesity outcomes in early
childhood. BMC Obes 2019;6:17. Crossref
11. Vereecken C, Haerens L, De Bourdeaudhuij I, Maes L. The
relationship between children’s home food environment
and dietary patterns in childhood and adolescence. Public
Health Nutr 2010;13:1729-35. Crossref
12. Rex SM, Kopetsky A, Bodt B, Robson SM. Relationships
among the physical and social home food environments,
dietary intake, and diet quality in mothers and children. J
Acad Nutr Diet 2021;121:2013-20.e1. Crossref
13. Chang HH, Nayga RM Jr. Mother’s nutritional label use
and children’s body weight. Food Policy 2011;36:171-8. Crossref
14. Nepper MJ, Chai W. Associations of the home food
environment with eating behaviors and weight status
among children and adolescents. J Nutr Food Sci
2015(S12):1-5. Crossref
15. Patrick H, Nicklas TA. A review of family and social
determinants of children’s eating patterns and diet quality.
J Am Coll Nutr 2005;24:83-92. Crossref
16. Coppinger T, Milton K, Murtagh E, et al. Global Matrix
3.0 Physical Activity Report Card for Children and Youth: a
comparison across Europe. Public Health 2020;187:150-6. Crossref
17. Huang WY, Wong SH, Sit CH, et al. Results from the Hong
Kong’s 2018 Report Card on physical activity for children
and youth. J Exerc Sci Fit 2019;17:14-9. Crossref
18. Barnes JD, Colley RC, Tremblay MS. Results from the
Active Healthy Kids Canada 2011 Report Card on Physical
Activity for Children and Youth. Appl Physiol Nutr Metab
2012;37:793-7. Crossref
19. Tremblay MS, Barnes JD, Bonne JC. Impact of the Active
Healthy Kids Canada report card: a 10-year analysis. J Phys
Act Health 2014;11 Suppl 1:S3-20. Crossref
20. De Villiers A, Steyn N, Coopoo Y, et al. Healthy Active
Kids. South Africa Report Card 2010. 2010. Available
from: https://www.activehealthykids.org/wp-content/uploads/2017/03/south-africa-report-card-long-form-2010.pdf. Accessed 5 Jul 2022.
21. Draper CE, Tomaz SA, Bassett SH, et al. Results from
the Healthy Active Kids South Africa 2018 Report Card.
SAJCH 2019;13:130-6. Crossref
22. Draper C, Basset S, de Villiers A, Lambert EV; HKKSA
Writing Group. Results from South Africa’s 2014 Report
Card on Physical Activity for Children and Youth. J Phys
Act Health 2014;11 Suppl 1:S98-104. Crossref
23. Aubert S, Barnes JD, Abdeta C, et al. Global Matrix 3.0
Physical Activity Report Card grades for children and
youth: results and analysis from 49 countries. J Phys Act
Health 2018;15:S251-73. Crossref
24. Tremblay MS, Gray CE, Akinroye K, et al. Physical activity
of children: a global matrix of grades comparing 15
countries. J Phys Act Health 2014;11 Suppl 1:S113-25. Crossref
25. Family Health Service, Department of Health, Hong Kong
SAR Government. Healthy eating for preschool children (2
years to 5 years old). 2022. Available from: https://www.fhs.gov.hk/english/health_info/child/12185.html. Accessed 5 Jul 2022.
26. Centre for Health Protection, Department of Health, Hong
Kong SAR Government. Nutrition guidelines for children
aged 2 to 6. Revised 2018. Available from: https://www.startsmart.gov.hk/files/pdf/nutritional_guide_en.pdf. Accessed 5 Jul 2022.
27. United Nations World Food Programme. Food
consumption score nutritional quality analysis (FCS-N)
guidelines. 2015. Available from: https://docs.wfp.org/api/documents/WFP-0000007074/download/. Accessed 5 May 2022.
28. Bui C, Lin LY, Wu CY, Chiu YW, Chiou HY. Association
between emotional eating and frequency of unhealthy food
consumption among Taiwanese adolescents. Nutrients
2021;13:2739. Crossref
29. Family Health Service, Department of Health, Hong Kong
SAR Government. Healthy eating for 6 to 24 month old
children (3) ready to go (12-24 months). 2022. Available
from: https://www.fhs.gov.hk/english/health_info/child/16301.html. Accessed 5 Jul 2022.
30. Centre for Health Protection, Department of Health, Hong
Kong SAR Government. Ideas for healthy cooking. 2017.
Available from: https://www.chp.gov.hk/en/static/90039.html. Accessed 5 Jul 2022.
31. Family Health Service, Department of Health, Hong Kong
SAR Government. Do your 0-5-years old children need
electronic screen products? 2022. Available from: https://www.fhs.gov.hk/english/health_info/child/30047.html. Accessed 5 Jul 2022.
32. Shim JE, Kim J, Mathai RA; STRONG Kids Research
Team. Associations of infant feeding practices and picky
eating behaviors of preschool children. J Am Diet Assoc 2011;111:1363-8. Crossref
33. Lo K, Cheung C, Lee A, Tam WW, Keung V. Associations
between parental feeding styles and childhood eating
habits: a survey of Hong Kong pre-school children. PLoS
One 2015;10:e0124753. Crossref
34. Yeung S, Chan R, Li L, Leung S, Woo J. Bottle milk feeding
and its association with food group consumption, growth
and socio-demographic characteristics in Chinese young
children. Matern Child Nutr 2017;13:e12341. Crossref
35. Family Health Service, Department of Health, Hong Kong
SAR Government. Healthy eating for infants and young
children—milk feeding. 2022. Available from: https://www.fhs.gov.hk/english/health_info/child/12549.html. Accessed 5 Aug 2022.
36. Wong EM, Sit JW, Tarrant MA, Cheng MM. The
perceptions of obese school children in Hong Kong toward
their weight-loss experience. J Sch Nurs 2012;28:370-8. Crossref
37. Ma G. Food, eating behavior, and culture in Chinese
society. J Ethn Foods 2015;2:195-9. Crossref
38. Nowicka P, Keres J, Ek A, Nordin K, Sandvik P. Changing
the home food environment: parents’ perspectives four
years after starting obesity treatment for their preschool
aged child. Int J Environ Res Public Health 2021;18:11293. Crossref
39. Fulkerson JA, Neumark-Sztainer D, Story M, et al. The
Healthy Home Offerings via the Mealtime Environment
(HOME) Plus study: design and methods. Contemp Clin
Trials 2014;38:59-68. Crossref
40. Fulkerson JA, Friend S, Horning M, et al. Family home
food environment and nutrition-related parent and child
personal and behavioral outcomes of the Healthy Home
Offerings via the Mealtime Environment (HOME) Plus
program: a randomized controlled trial. J Acad Nutr Diet
2018;118:240-51. Crossref
41. Olstad DL, Raine KD, Nykiforuk CI. Development of a
report card on healthy food environments and nutrition
for children in Canada. Prev Med 2014;69:287-95. Crossref
42. Wan AW, Chung KK, Li JB, Xu SS, Chan DK. An assessment
tool for the international healthy eating report card for
preschool-aged children: a cross-cultural validation across
Australia, Hong Kong, Singapore, and the United States.
Front Nutr 2024;11:1340007. Crossref
43. Chan DK, Ivarsson A, Stenling A, Yang SX, Chatzisarantis NL,
Hagger MS. Response-order effects in survey methods: a
randomized controlled crossover study in the context of
sport injury prevention. J Sport Exerc Psychol 2015;37:666-73. Crossref
44. Chan DK, Stenling A, Yusainy C, et al. Editor’s Choice:
Consistency tendency and the theory of planned behavior:
a randomized controlled crossover trial in a physical
activity context. Psychol Health 2020;35:665-84. Crossref