Hong Kong Med J 2022 Apr;28(2):175–7 | Epub 17 Mar 2022
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
CASE REPORT
COVID toe in an adolescent boy: a case report
Joshua SC Wong, MB, BS, FHKAM (Paediatrics)1 †; TS Wong, MB, ChB, MRCPCH1 †; Gilbert T Chua, MB, BS, FHKAM (Paediatrics)2 †; Christy Wan, MB, BS1; SH Lau, MB, BS1; Samuel CS Ho, MB, BS1;
Jaime S Rosa Duque, MD, PhD2; Ian CK Wong, PhD, FRCPCH3,4; Kelvin KW To, MD, FRCPath5; Winnie WY Tso, FHKAM (Paediatrics)2; Christine S Wong, MRCP, FHKCP6; Marco HK Ho, MD, FHKAM (Paediatrics)2; Janette Kwok, PhD, FRCPA7; CB Chow, MD, FHKAM (Paediatrics)1; Paul KH Tam, FRCS, FRCPCH8,9; Godfrey CF Chan, MD, FRCPCH,2; WH Leung, MD, PhD2; YL Lau, MD, FRCPCH2; Patrick Ip, MPH, FHKAM (Paediatrics)2; Mike YW Kwan, MSc (Applied Epidemiology) CUHK, FHKAM (Paediatrics)1
1 Department of Paediatrics and Adolescent Medicine, Princess Margaret Hospital, Hong Kong
2 Department of Paediatrics and Adolescent Medicine, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Hong Kong
3 Centre for Safe Medication Practice and Research, Department of Pharmacology and Pharmacy, The University of Hong Kong, Hong Kong
4 Research Department of Practice and Policy, UCL School of Pharmacy, University College London, United Kingdom
5 Department of Microbiology, Carol Yu Centre for Infection, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Hong Kong
6 Dermatology Division, Department of Medicine, Queen Mary Hospital, Hong Kong
7 Division of Transplantation and Immunogenetics, Department of Pathology, Queen Mary Hospital, Hong Kong
8 Division of Paediatric Surgery, Department of Surgery, The University of Hong Kong, Hong Kong
9 Dr Li Dak-Sum Research Centre, The University of Hong Kong–Karolinska Institutet Collaboration in Regenerative Medicine, The University of Hong Kong, Hong Kong
† Co-first authors
Corresponding author: Dr Mike YW Kwan (kwanyw1@ha.org.hk)
 Full paper in PDF
Full paper in PDF
Case report
In July 2020, a 17-year-old Pakistani boy presented
with pain in his right foot unrelated to trauma
or insect bite, after returning from Pakistan. The
following day he tested positive for severe acute
respiratory syndrome coronavirus 2 (SARS-CoV-2)
infection. He had no previous medial history but
was obese with a body mass index of 32.4 kg/m2.
He denied any camping, water-trekking, or outdoor
barefoot walking while in Pakistan. Physical
examination revealed multiple purplish, flat, dry
lesions <5 mm in diameter on his right toes and
dorsum of the foot. They were tender on palpation
but there was no surrounding erythema (Fig). No
lesions were evident on the left foot or elsewhere
and he had no symptoms or signs suggestive of any
systemic autoimmune disorder. Pain associated
with the lesions subsided by day 4 of illness. Some
lesions spontaneously resolved but some became
raised and crusted after day 3 (Fig). Topical fusidic
acid for 1 week was prescribed to treat any potential
bacterial infection. Of note, he developed a fever
up to 39°C on day 8 and a productive cough. Vital
signs remained stable with no respiratory distress
or need for oxygen therapy. Chest X-ray did not
show pneumonic changes and fever subsided within
24 hours. White blood cell count and differential were
normal and C-reactive protein was 28 mg/L. Alanine
aminotransferase was initially elevated at 131 U/L
but showed a downward trend on rechecking.
Clotting profile and D-dimer were normal. On day 12, SARS-COV-2 immunoglobulin G was detected
and the patient was discharged from the hospital.
His toe lesions resolved completely a few days later.
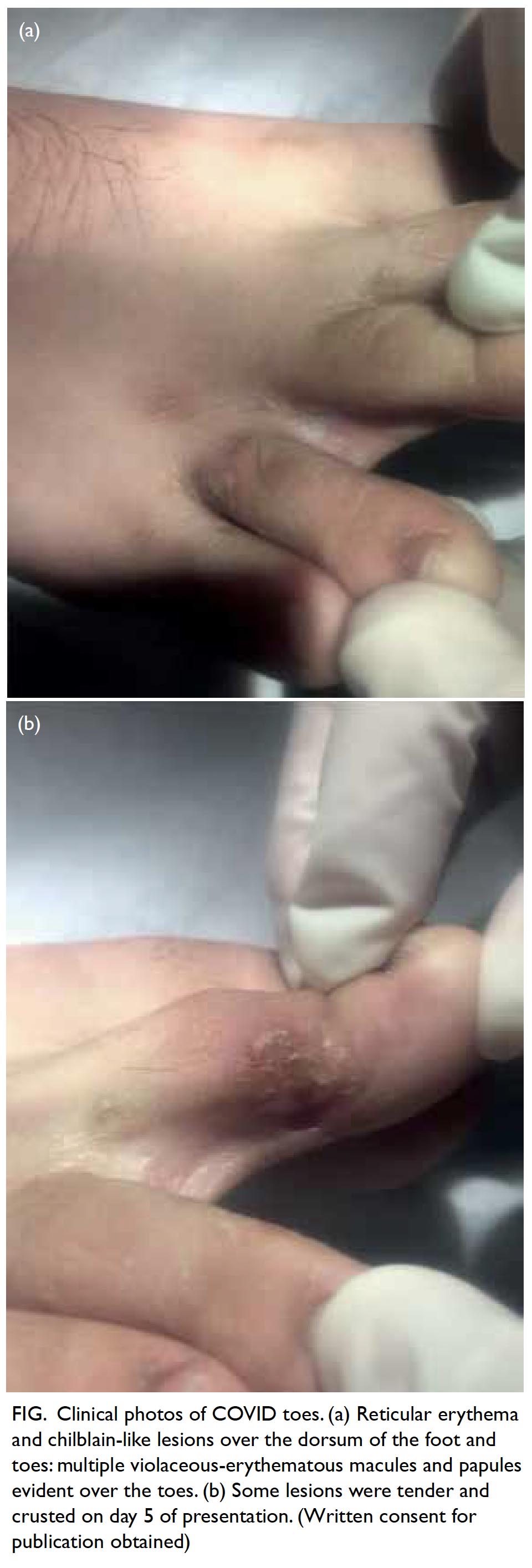
Figure. Clinical photos of COVID toes. (a) Reticular erythema and chilblain-like lesions over the dorsum of the foot and toes: multiple violaceous-erythematous macules and papules evident over the toes. (b) Some lesions were tender and crusted on day 5 of presentation. (Written consent for publication obtained)
Discussion
Rash is an uncommon symptom in coronavirus
disease 2019 (COVID-19) infection.1 It has been
described in Italy where 20% of COVID-19 patients
developed cutaneous signs, including erythematous
rash and widespread urticarial or vesicular lesions,
at disease onset or following hospitalisation. The
lesions usually subsided after a few days and there
was no correlation with disease severity.2 Cutaneous
manifestations included pseudo-chilblain (pernio-like),
vesicular eruptions, urticarial lesions,
maculopapular eruptions, and livedo or necrosis.2 3
Classic chilblains (or pernios) are
inflammatory skin lesions that occur on the dorsal
surface of the fingers and toes. They form painful
and itchy erythematous and oedematous nodules
that may ulcerate. They are triggered by cold and
usually recur yearly during winter.3 Since March
2020, cases of acral lesions resembling chilblains
have been reported across Europe, coinciding with
the beginning of the COVID-19 outbreak. These
lesions have differed to classic ones, showing an
equal sex distribution, absence of obvious triggering
factors, and involvement of the feet and distal third
of the legs.3 They have been seen more commonly
in previously healthy children or adolescents aged
>10 years, almost always (74%-100%) on the feet but occasionally on the hands and fingers. The lesions
were multiple and varied in size from a few millimetres
to centimetres and were described as erythematous,
violaceous, swollen, or purpuric. Itchiness and
mild pain were frequently reported but required
only symptomatic treatment. Lesions started to
regress within 12 days to 8 weeks with complete
resolution. The appearance of chilblain-like lesions
was not thought to be associated with a poor disease
outcome.2 3 A major limitation of these reports is
that only 11% of cases hospitalised tested positive for
SARS-CoV-2 by polymerase chain reaction (PCR),
with the remainder untested or testing negative.
Some authors have attributed this to the low
sensitivity of tests or low viral load in children.3 The
pathophysiological relationship between COVID-19
infection and chilblain-like lesions remains poorly
understood, but has been hypothesised to be related
to type 1 interferonopathies.3
Our patient is one of the few reported cases
of laboratory-confirmed SARS-CoV-2 infection
with chilblain-like lesions. To date, our patient
is the only child in Hong Kong to present with
SARS-CoV-2 infection as well as so-called “COVID
toe”.1 Currently, there are insufficient data to
determine a clear relationship between these
dermatological symptoms and COVID-19. Rash is
a common manifestation of many diseases and may
not be associated COVID-19 infection. A recent
case series of 17 adolescents in Italy who developed
chilblain-like lesions during the first wave of
COVID-19 screened negative on SARS-CoV-2 PCR
of nasopharyngeal swabs, negative for SARS-CoV-2
immunoglobulin M and immunoglobulin G, and had
no viral genome in biopsy specimens. However,
this report was limited by its small sample size and
did not compare data with an age- and gender-standardised
background incidence of chilblains in
the population.4 Most patients with dermatological
manifestations were not confirmed to be infected
with SARS-CoV-2. Another systematic review also
concluded that some, but not all paediatric cases,
who developed chilblain-like lesions during the
COVID-19 pandemic had positive SARS-CoV-2
PCR, serology or viral particles confirmed in
electron microscopy.5 Larger-scale epidemiological
study is needed to confirm an association between
these chilblain-like lesions and COVID-19
infection. Reported manifestations and histological
findings were too heterogeneous to ascertain the
pathophysiology. Nevertheless, physicians should
remain vigilant since dermatological manifestations
may be the first or only symptom in patients with
COVID-19 infection,2 3 enabling a timely diagnosis
of COVID-19 infection to reduce transmission.
Physicians should also consider the possibility of
coagulopathies and interferonopathies.
Author contributions
Concept or design: MYW Kwan, P Ip.
Acquisition of data: C Wan, SH Lau, SCS Ho, JS Rosa Duque.
Analysis or interpretation of data: C Wan, SH Lau, SCS Ho, JS Rosa Duque.
Drafting of the manuscript: JSC Wong, TS Wong, GT Chua.
Critical revision of the manuscript for important intellectual content: ICK Wong, KKW To, WWY Tso, CS Wong, MHK Ho, J Kwok, CB Chow, PKH Tam, GCF Chan, WH Leung, YL Lau.
Acquisition of data: C Wan, SH Lau, SCS Ho, JS Rosa Duque.
Analysis or interpretation of data: C Wan, SH Lau, SCS Ho, JS Rosa Duque.
Drafting of the manuscript: JSC Wong, TS Wong, GT Chua.
Critical revision of the manuscript for important intellectual content: ICK Wong, KKW To, WWY Tso, CS Wong, MHK Ho, J Kwok, CB Chow, PKH Tam, GCF Chan, WH Leung, YL Lau.
All authors approved the final version of the manuscript and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding/support
This study is supported by the Collaborative Research Fund (CRF) 2020/21 and One-off CRF Coronavirus and Novel
Infectious Diseases Research Exercises (Ref: C7149-20G).
The funders had no role in study design, data collection
and analysis, decision to publish, or preparation of the
manuscript.
Ethics approval
The patient was treated in accordance with the Declaration of Helsinki, provided informed consent for the treatment/procedures, and provided consent for publication.
References
1. Chua GT, Wong JS, Lam I, et al. Clinical characteristics and
transmission of COVID-19 in children and youths during
3 waves of outbreaks in Hong Kong. JAMA Network Open
2021;4:e218824. Crossref
2. Andina D, Belloni-Fortina A, Bodemer C, et al. Skin
manifestations of COVID-19 in children: Part 2. Clin Exp
Dermatol 2021;46:451-61. Crossref
3. Andina D, Belloni-Fortina A, Bodemer C, et al. Skin
manifestations of COVID-19 in children: Part 1. Clin Exp
Dermatol 2021;46:444-50. Crossref
4. Discepolo V, Catzola A, Pierri L, et al. Bilateral chilblain-like
lesions of the toes characterized by microvascular
remodeling in adolescents during the COVID-19
pandemic. JAMA Network Open 2021;4:e2111369. Crossref
5. Koschitzky M, Oyola RR, Lee-Wong M, Abittan B, Silverberg N. Pediatric COVID toes and fingers. Clin
Dermatol 2021;39:84-91. Crossref