Hong Kong Med J 2017 Oct;23(5):480–8 | Epub 25 Aug 2017
DOI: 10.12809/hkmj166143
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
ORIGINAL ARTICLE
Occupational stress and burnout among Hong Kong dentists
HB Choy, MGD (CDSHK), MRACDS (GDP)1;
May CM Wong, MPhil, PhD2
1 Dentistry and Maxillofacial Surgery, Caritas Medical Centre,
Shamshuipo, Hong Kong
2 Faculty of Dentistry, The University of Hong Kong, Pokfulam, Hong Kong
Corresponding author: Dr May CM Wong (mcmwong@hku.hk)
An earlier version of this paper was presented at the 94th General Session
& Exhibition of the IADR, 3rd Meeting of the IADR Asia Pacific Region and
35th Annual Meeting of the IADR Korean Division held in Seoul, Korea on
22-25 June 2016.
 Full
paper in PDF
Full
paper in PDF
Abstract
Introduction: Professional burnout has been
described as a gradual erosion of a person and may
be one of the possible consequences of chronic
occupational stress. Although occupational stress
has been surveyed among dentists in Hong Kong,
no study has been published about burnout in the
profession. This study aimed to evaluate burnout
among Hong Kong dentists and its association with
occupational stress.
Methods: We surveyed a random sample of 1086
registered dentists in Hong Kong, which formed
50% of the local profession. They were mailed
an anonymous questionnaire about burnout and
occupational stress in 2015. The questionnaire
assessed occupational stress, coping strategies,
effects of stress, level of burnout, and socio-demographic
characteristics of the respondents.
Occupational stress assessment concerned 33
stressors in five groups: patient-related, time-related,
income-related, job-related, and staff-/technically
related. Level of burnout was assessed by the Maslach
Burnout Inventory–Human Services Survey (22
items) with three scores: emotional exhaustion,
depersonalisation, and personal accomplishment.
Results: Completed questionnaires were received
from 301 dentists (response rate, 28.3%), of whom
25.4% had a high level of emotional exhaustion,
17.2% had a high level of depersonalisation, and 39.0% had a low level of personal accomplishment.
Only 7.0% of respondents, however, had a high
level of overall burnout (high emotional exhaustion,
high depersonalisation, and low personal
accomplishment). A high level of overall burnout
was significantly associated with a higher mean score
for job-related stressors and lack of postgraduate
qualifications (P<0.05).
Conclusions: Patient-related stressors are the top
occupational stressors experienced by dentists in
Hong Kong. In spite of this, a low proportion of
dentists have a high level of overall burnout. There
was a positive association between occupational
stress and level of burnout.
New knowledge added by this study
- Approximately 7.0% of Hong Kong dentists have a high level of overall burnout.
- Job-related stressors and postgraduate qualifications are associated with a high level of overall burnout.
- Although only a low proportion of Hong Kong dentists has high overall burnout, this issue should not be overlooked. Dentistry is quite a lonely profession. Peer support and sharing is important for the development of dentistry in Hong Kong.
- Dentists are advised to update their knowledge and skills to meet the increasing expectations and challenges from patients and the society.
Introduction
Professional burnout can be one of the possible
consequences of chronic occupational stress.1
Burnout has been described as a gradual erosion
of the person and comprises three characteristics.2
First, the individuals are exhausted, either
mentally or emotionally.2 They feel drained, tired
with insufficient energy, and are unable to cope.3
Second, they may have a negative, indifferent,
or cynical attitude towards patients, clients, or
colleagues.2 They feel numb about work and distance
themselves emotionally.3 Finally, they also tend to
feel dissatisfied with their own performance and
evaluate themselves negatively.2 They find difficulty
in concentrating on their work and caring about
their families.3 The consequences of burnout can be
very serious. Maslach and Jackson4 found that the
quality of care and service provided by individuals
who have burnout syndrome may be substandard.
Burnout has also been found to be associated with
job turnover, absenteeism, low morale, and personal
dysfunction.3 Maslach and her colleague5 6 have
studied the burnout syndrome for many years and
devised a measurement tool—the Maslach Burnout
Inventory—Human Services Survey (MBI-HSS).4 7 Although some studies of burnout have been
conducted among dentists using the MBI-HSS,1 8 9 10
most studies on stress and burnout in health
professions have focused on physicians11 12 13and
nurses.14 15
In 2001, a survey was conducted to investigate
the sources of occupation stress among dentists in
Hong Kong.16 There has been no published study on
burnout among dentists in Hong Kong since then.
We conducted a cross-sectional study to investigate
the burnout among dentists in Hong Kong and
the association between occupational stress and
burnout. The objectives of our study were to identify
the occupational stressors and the prevalence of
burnout among dentists in Hong Kong and their
association.
Methods
Survey design and sample
In October 2015, there were 2173 locally registered
dentists working in Hong Kong according to the
Dental Council of Hong Kong.17 In order to achieve
the width of the 95% confidence interval (CI)
calculated from the sample proportion estimates
of burnout outcomes no wider than ± 5%, a sample
of 384 dentists was needed (using a conservative
assumption of sample proportions to be 50%).
Taking into account the low response rate (<40%)
achieved by previous surveys in Hong Kong,
50% of the dentists were systematically randomly
sampled (with a random start of ‘2’ generated from
Excel) from the published list of registered dentists
according to their family names and a sample size of
1086 was chosen. The questionnaires were mailed in
sealed envelopes in early November 2015 along with
a stamped, self-addressed envelope. The participants
were assured of confidentiality. No names and
addresses were asked for and no codes were
marked on the questionnaires or return envelopes.
Questionnaires for selected government dentists
were sent collectively to the Department of Health
and delivered internally. Reminders were sent to all
selected private dentists in late November or early
December 2015. Participants did not receive any
specific incentive to complete this survey.
Construction of questionnaire
The questionnaire assessed the sources of
occupational stress, stress-coping strategies, effects
of stress on work, level of burnout, and socio-demographic
characteristics of the study subjects.
There were 33 occupational stressors for identifying
the sources of stress; 26 of which were proposed by
Cooper et al.18 An additional seven stressors were
proposed by Waddington.19 Participants were asked
to rate the level of stress they experienced on a
5-point scale ranging from ‘1 = No stress’ to ‘5 = A
great deal of stress’. The 33 stressors were grouped
into five domains: patient-related, time-related,
income-related, job-related, and staff-related or
technically related (Box). Based on the work by
Cooper et al,18 10 stress-coping strategies of dentists
were included. Participants were asked how often
they would use these stress-coping strategies with
responses categorised on a 5-point scale ranging
from ‘1 = Never’ to ‘5 = Always’ (Box). Based on
the work of Kopec and Esdaile,20 five effects of
occupational stress on work were included with
responses rated on a 4-point scale ranging from ‘1 =
Not at all’ to ‘4 = A lot’ (Box). Of note, MBI-HSS,7
which has been recognised as the leading measure of
burnout, was also included and consisted of 22 items
with responses rated on a 7-point scale ranging from
‘0 = Never’ to ‘6 = Every day’. The MBI-HSS addressed
three general scales: emotional exhaustion (EE; 9
items with score range of 0-54) measuring the feelings
of being emotionally overextended and exhausted
by one’s work; depersonalisation (DP; 5 items with
score range of 0-30) measuring the unfeeling and
impersonal response towards recipients of one’s
service, care treatment, or instruction; and personal
accomplishment (PA; 8 items with score range of
0-48) measuring the feelings of competence and
successful achievement in one’s work. Personal
information about the participants was also collected
and included their age, gender, years of practice,
type of practice, location, hours of work per week,
marital status, working status of spouse, number of
children, religious beliefs, whether the participant
had postgraduate qualifications, and whether the
participant was a specialist.
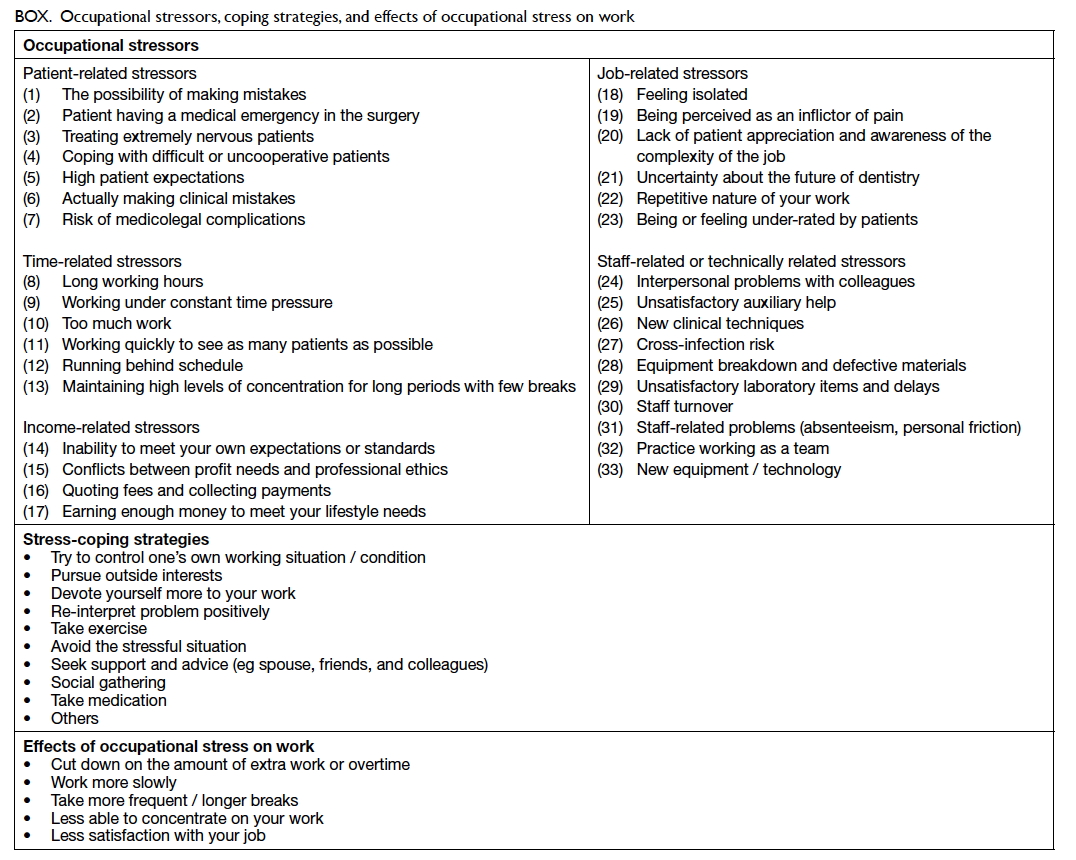
Box. Occupational stressors, coping strategies, and effects of occupational stress on work
The Institutional Review Board of The
University of Hong Kong/Hospital Authority Hong
Kong West Cluster (HKU/HA HKW IRB, reference
number: UW 15-524) approved the study prior to
distribution of the questionnaires.
Statistical analysis
The mean score for each stressor group was calculated
and ranked. Three subscale scores of MBI-HSS (EE,
DP, and PA) were calculated and subjects categorised
into one of the three groups—high, moderate, or low
level of burnout. Those with EE score of ≥27 were
considered to have high EE level, 17-26 moderate
and 0-16 low level. Those with DP score of ≥13 were
considered to have high DP level, 7-12 moderate
and 0-6 low level. Those with PA score of ≤31 were
considered to have low PA level, 32-38 moderate
and ≥39 high level. Subjects with high EE, high DP,
and low PA levels simultaneously were considered
to have a high level of overall burnout. Others were
considered to have low overall burnout. Of the
results, 95% CIs were computed as well.
The relationships between EE, DP and PA
scores, and the set of 17 independent variables (12
demographic variables and the five stressor group
scores) were analysed by analysis of covariance
(ANCOVA). A forward selection method was
adopted. In this approach, independent variables
were added into the model one at a time. In each
step, each variable that was not already in the model
was tested for inclusion in the model. The most
significant of these variables was added to the model.
Finally, only significant variables were selected in the
final model.
The relationship between levels of overall
burnout (high and low) and the set of 17 independent
variables was analysed by multiple logistic regression.
A forward selection method was adopted as well. All
analyses were performed using the SPSS (Windows
version 22.0; IBM Corp, Armonk [NY], US) and the
level of significance was set at 0.05.
Results
Response
A total of 1086 questionnaires were sent to the
randomly selected dentists. Reminders were sent
to the selected private dentists 2 to 4 weeks later.
We received 301 completed questionnaires and 22
questionnaires returned undelivered by the post
office, resulting in a response rate of 28.3% (301/[1086–22] x 100%).
Demographics
The demographics of the respondents are shown
in Table 1. Approximately 65% of the respondents
were male and 79% worked in the private sector
that also included non-governmental organisations.
Approximately 46% of dentists had acquired one or
more postgraduate qualifications. More than 86% of
the respondents were general dental practitioners.
Over a quarter (29%) had never married and more
than half (54%) claimed to have no religious beliefs.
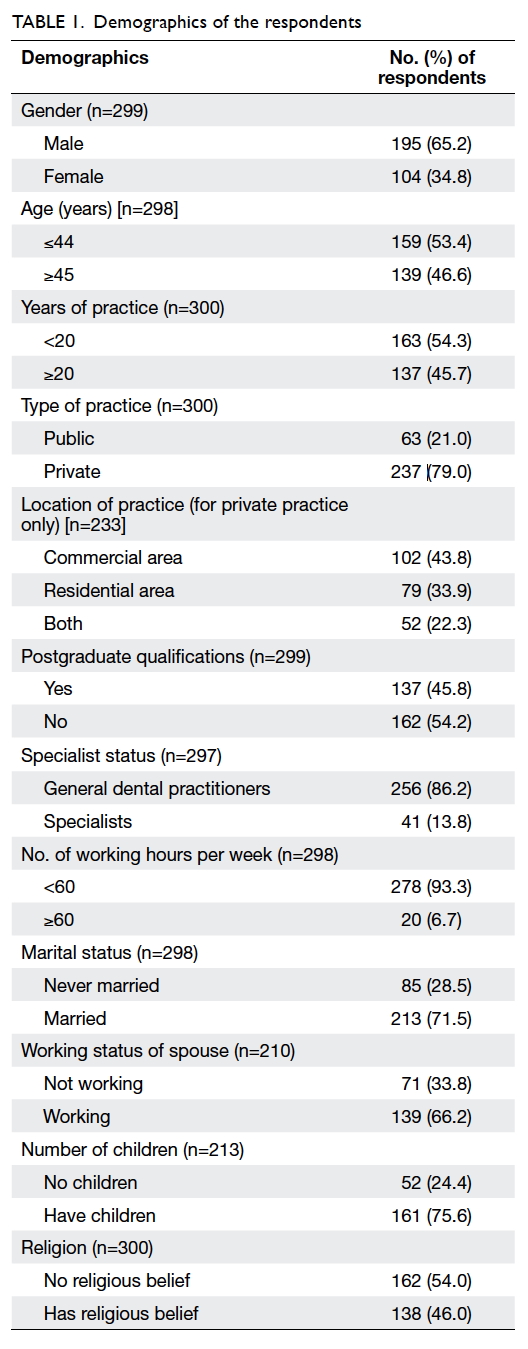
Table 1. Demographics of the respondents
Occupational stress
The top 10 stressors according to the percentage
distribution of the respondents’ ratings ‘4’ or ‘5’
(considered to be high level) are shown in Figure 1. Six of the top 10 highest ranked stressors (and
actually the top five highest ranked) were patient-related
stressors and three of the 10 highest ranked
stressors were time-related. The patient-related
stressors group had the highest mean (± standard
deviation [SD]) score (3.4 ± 0.8), followed by the
time-related stressors group (3.1 ± 0.8), staff-related
or technically related stressors group (2.6 ± 0.6),
income-related stressors group (2.5 ± 0.7), and job-related
stressors group (2.5 ± 0.7). Female dentists
had a higher mean score than male dentists for
patient-related, job-related, and staff-/technically
related stressors (3.5 vs 3.3, 2.6 vs 2.4, and 2.7 vs 2.5,
respectively; all P<0.05). Dentists with more than
20 years of practice (3.3), who held postgraduate
qualifications (3.2), or who had completed specialist
training (3.0) had a lower mean score for patient-related
stressors than those with less than 20 years
of practice (3.4, 3.5, and 3.4 respectively; all P<0.05).
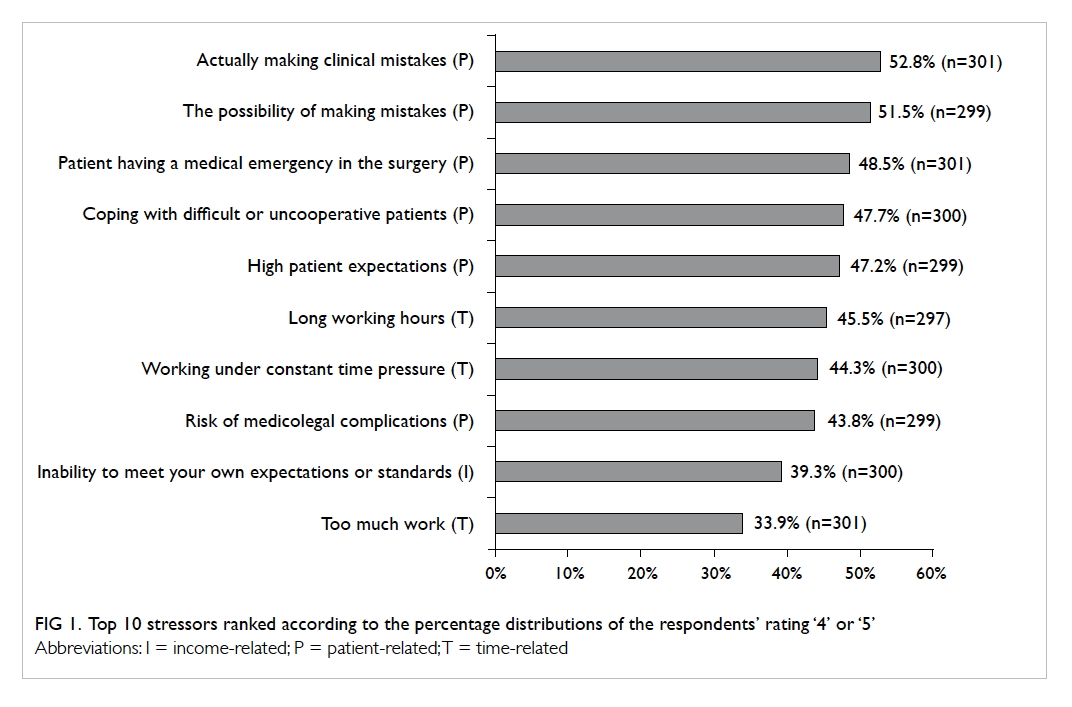
Figure 1. Top 10 stressors ranked according to the percentage distributions of the respondents’ rating ‘4’ or ‘5’
Stress-coping strategies
The highest ranked strategy (with ratings ‘4’ or ‘5’)
to cope with occupational stress was ‘try to control
one’s own working situation / condition’ (59.0%),
followed by ‘pursue outside interests’ (58.6%), ‘avoid
the stressful situation’ (51.7%), and ‘take exercise’
(51.0%). Other less-commonly used strategies (<50%)
were ‘re-interpret problem positively’, ‘seek support
and advice’, ‘social gathering’, ‘devote yourself more
to your work’, ‘take medication’, and ‘others’.
Effects of occupational stress on work
The highest ranked effect (with ratings ‘3’ or ‘4’) of
occupational stress on work was to ‘cut down on
the amount of extra work or overtime’ (41.7%) and
‘take more frequent / longer breaks’ (30.7%). Fewer
than 30% of respondents reported ‘less satisfaction
with your job’, ‘work more slowly’, and ‘less able
to concentrate on your work’ as the effects of
occupational stress on work.
Maslach Burnout Inventory–Human Services
Survey and level of burnout
The mean (± SD) score for EE, DP and PA and the
level of burnout are shown in Figure 2. Approximately
a quarter of the respondents had a high EE level
(25.4%; 95% CI, 20.5%-30.3%) while 17.2% (95% CI,
12.9%-21.5%) and 39.0% (95% CI, 33.5%-44.5%) had
high DP and low PA level, respectively. Nonetheless
only 7.0% (95% CI, 4.1%-9.9%) of respondents had
a high level of overall burnout (ie high EE, high DP,
and low PA).
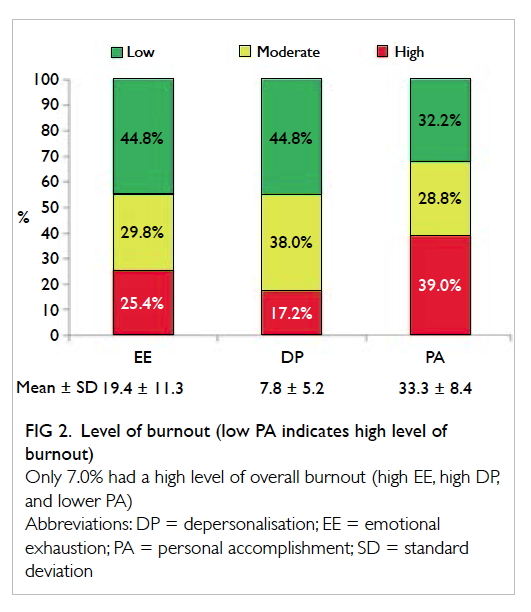
Figure 2. Level of burnout (low PA indicates high level of burnout)
Only 7.0% had a high level of overall burnout (high EE, high DP, and lower PA)
Maslach Burnout Inventory–Human
Services Survey, occupational stress, and
demographic variables
The relationship between EE, DP and PA scores, five
stressor groups, and the 12 demographic variables
was analysed by ANCOVA. The final models are
shown in Table 2. For EE, among the 17 independent
variables investigated, only three significant
variables (P<0.05) were selected in the final model.
The dentists whose spouses were not working had a
higher mean EE score by 4.15 compared with those
whose spouses were working (P=0.024). Those with
higher scores in the time-related stressors group
had higher EE scores. For every one unit increase
in time-related stressors group score, the mean EE
score increased by 4.51 (P<0.001). Finally, those with
higher scores in the job-related stressors group also
had higher EE scores; for every one unit increase
in job-related stressors group score, the mean EE
score increased by 4.54 (P<0.001). For DP, only
two significant variables (P<0.05) were selected
in the final model. Private dentists who worked in
residential areas had higher mean DP scores by 2.51
compared with those private dentists who worked
in commercial areas (P=0.005). Also, those with
higher scores in the job-related stressors group also
had higher DP scores; for every one unit increase
in job-related stressors group score, the mean DP
score increased by 2.35 (P<0.001). For PA, only one
significant variable (P<0.05) was selected in the final
model. Those with higher scores in income-related
stressors group were found to have lower PA scores.
For every one unit increase in job-related stressors
group score, the mean PA score decreased by 3.40
(P<0.001).
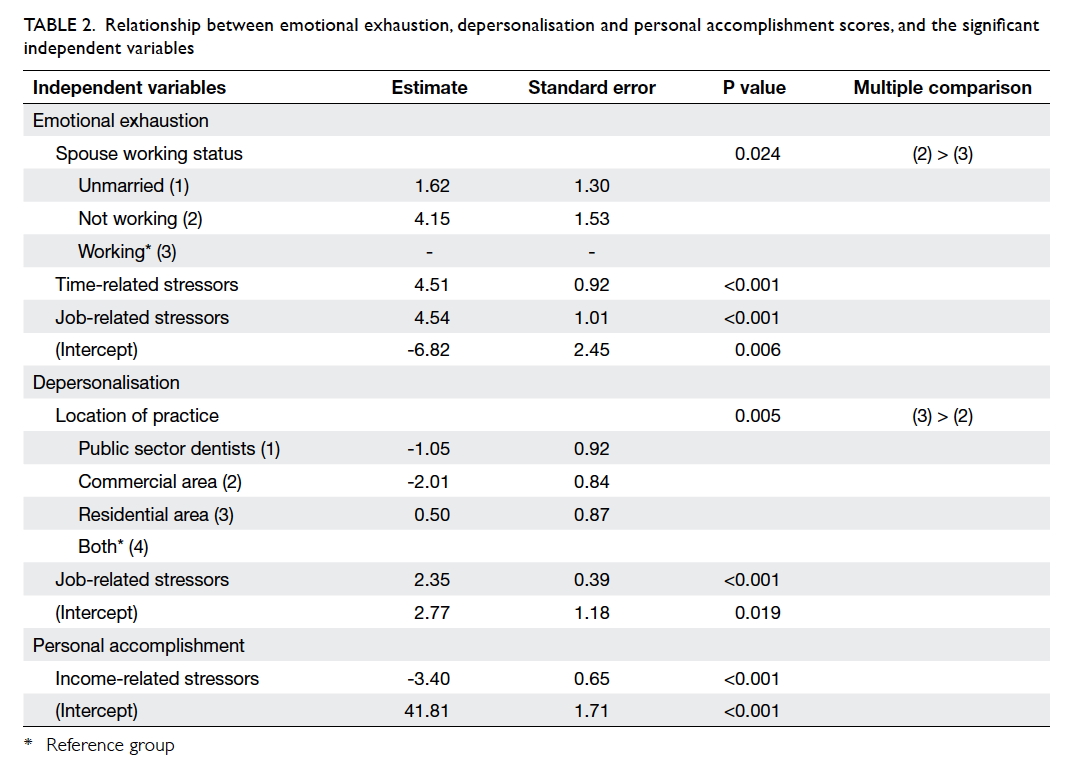
Table 2. Relationship between emotional exhaustion, depersonalisation and personal accomplishment scores, and the significant independent variables
Level of burnout, occupational stress, and
demographic variables
The relationships between levels of overall burnout
(high and low), five stressors groups, and the
demographic variables were analysed by multiple
logistic regression. The results are shown in Table 3;
only two significant variables (P<0.05) were selected.
The chance of having a high level of overall burnout
among dentists with no postgraduate qualifications
was 5.08 times higher (95% CI, 1.09-23.61) than those with postgraduate qualifications (P=0.038).
Also, for every one unit increase in job-related
stressors group score, the odds of having a high level
of overall burnout was 3.74 times as likely (95% CI,
1.77-7.87; P=0.001).
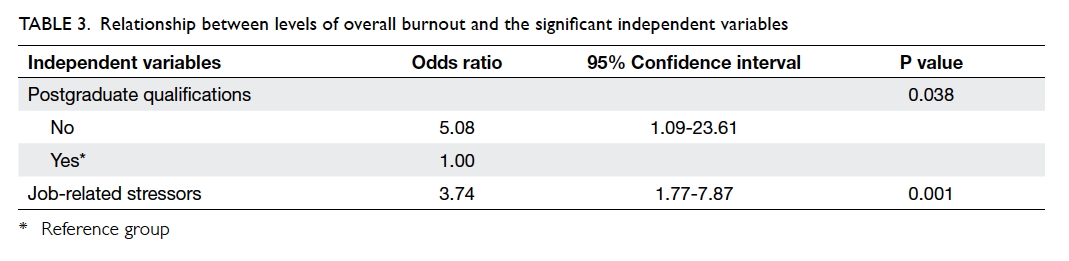
Table 3. Relationship between levels of overall burnout and the significant independent variables
Discussion
This survey revealed that the highest ranked
stressors were patient-related. Several stress-coping
strategies and effects of occupational stress on work
were identified. Only 7% of dentists had a high level
of overall burnout. Dentists without postgraduate
qualifications and higher job-related stressor scores
were more likely to have a high level of overall
burnout.
Occupational stress and coping strategies
Comparison of these results with those of a previous
study published in 200116 reveals that the situation
in Hong Kong has changed little over 15 years. In
both surveys, six of the top 10 stressors were patient-related,
three were time-related, and one was income-related.
There was, however, an increase in the
percentage distributions of the stressors, indicating
an increased stress level for dentists in Hong Kong
in the past decade. This may be related to increasing
demands and expectations of patients. Patients can
now find much information on the internet and ask
many questions based on the information they may
find. This is a novel challenge for dentists. Moreover,
the property rents in Hong Kong have increased
much over the last 10 years with a consequent
increase in the overhead costs of running a dental
clinic. As a result, dentists need to work harder and
see more patients to generate sufficient income to
cover their costs.
Female dentists had higher mean scores than
male dentists for patient-related, job-related, and
staff-/technically related stressors. This may be
because they are taking care of their own family
as well as working as a dentist. Dentists with more
experience, higher postgraduate qualifications, and
specialist training had lower mean scores in the
patient-related stressors group. This may imply that
dentists with more competent skills and knowledge
were less stressed.
In the current and 200116 studies, the most
prevalent method of coping with stress was ‘try to
control one’s own working situation / condition.
Most dentists worked on their own and were self-reliant,
even when they were facing stress.
Maslach Burnout Inventory–Human Services
Survey and level of burnout
Higher EE score was significantly associated with
those dentists whose spouses were not working and
those with higher mean scores in time-related and
job-related stressors groups. The financial pressure
on a dentist may be lessened if the spouse works and
this may have contributed to the lower EE score.
Higher DP score was significantly associated with
working in a residential area and higher mean score
in job-related stressors group. This may be due to
differing patient profiles in residential areas. Those
who seek dental care from dentists in residential areas
may be less educated, and less willing or less able to
pay for dental treatment. Thus, the dentists have to
spend more time with each patient but accrue less
income with a consequent higher DP score. Lower
PA score was significantly associated with those
dentists with lower mean score in income-related
stressors group. One of the rewards for a dentist is
to earn a living by providing a professional dental
service. If a dentist has difficulty in earning, he may
have a lower sense of PA.
A high level of overall burnout was significantly
associated with a higher mean score in job-related
stressors group and no postgraduate qualifications.
Those with postgraduate qualifications may have
better knowledge, technique, and communication
skills to deal with patients. This may have contributed
to lower overall burnout.
The mean scores of the three subscales (EE,
DP, and PA) of MBI of studies in Korea,8 Northern
Ireland,9 UK,10 Dutch,21 and Hong Kong doctors11
are shown in Figure 3 for comparison. Generally
speaking, the mean scores of EE and DP of dentists
in Hong Kong were lower than those in other
countries while mean PA score was in between. It is
possible that Hong Kong dentists can tolerate stress
better. In Hong Kong, the competition to study
dentistry is very strong. A secondary school student
must perform very well in public examinations to be
admitted to the only dental school in Hong Kong.
Locally trained students are used to this kind of keen
competition. In Hong Kong, lower mean EE and DP
scores and higher mean PA scores among dentists
suggest that they are not as stressful as medical
doctors. This may be due to the different nature of
their jobs. Most dentists in Hong Kong practise in
the private sector and seldom need to be on-call.
In comparison, a lot of Hong Kong medical doctors
work in public hospitals and need to be on-call.
Moreover, the public have high expectations of the
public health care service and this may contribute
to the higher level of burnout among Hong Kong
doctors.
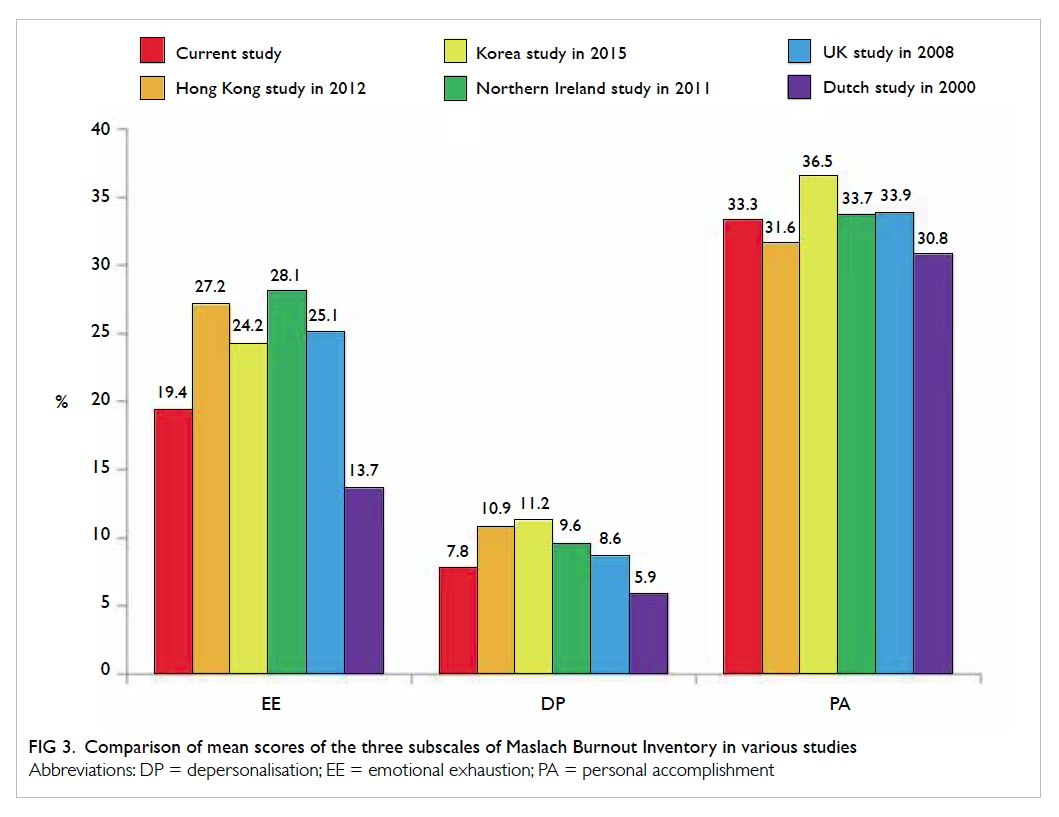
Figure 3. Comparison of mean scores of the three subscales of Maslach Burnout Inventory in various studies
The level of burnout of the current study was
compared with that reported in Korea8 and the UK.10
The percentage distribution of high EE (Hong Kong
25.4%, Korea 41.2%, and UK 42.2%) and DP (Hong
Kong 17.2%, Korea 55.9%, and UK 19.5%) level of
Hong Kong dentists was lower compared with that
of Korean and UK dentists. Hong Kong dentists,
however, felt a lower sense of PA as reflected by the
higher percentage of low PA (Hong Kong 39.0%,
Korea 31.5%, and UK 31.9%). This suggests that the
dentists in Hong Kong had lower job satisfaction.
Although the level of overall burnout of Hong Kong
dentists was less than that in other countries, this
issue should not be overlooked. Dentistry is quite a
lonely profession that requires an individual to work
alone most of the time. Peer support and sharing is
important for the development of dentistry in Hong
Kong.
Limitations of the study
The response rate of the current study was low
(<30%) although it was similar to other studies of
health care professionals in Hong Kong. The selected
dentists might be very busy and might not have time to
complete the questionnaires. Others might not have
been interested. Those dentists with a high level of
burnout might have felt the questions too sensitive
and thus been unwilling to participate. For those
who participated, as stress and burnout were self-reported,
there might have been information bias
because of social desirability and thus our results might
underestimate the level of stress and burnout among
dentists in Hong Kong. As in all cross-sectional
surveys, a causal relationship could not be established.
With the small sample size, there was a possible lack of
statistical power for the multiple logistic regression
as evidenced by the wide 95% CI of the odds ratio. In
order to increase the response rate of future surveys,
we may consider phoning each selected dentist to
check if they have received the questionnaires and
to invite them to participate. We may also consider
using the internet for data collection.
Recommendation
Dentists with a higher stress level may consider
working less to relieve pressure: approximately one
quarter of dentists worked more than 50 hours a
week, which contributed to the time-related stress.
Dentists are advised to update their knowledge and
skills to equip them for the increasing expectations
and challenges from patients and society.
Conclusion
Patient-related stressors are the top occupational
stressors experienced by dentists in Hong Kong.
Nonetheless a small proportion of dentists have high
overall burnout. There was a positive association
between occupational stress and level of burnout.
Acknowledgements
We would like to thank the staff of the Faculty of
Dentistry, The University of Hong Kong for their
assistance in this study. We would also like to thank
all the dentists who participated in the survey.
Declaration
All authors have disclosed no conflicts of interest.
References
1. Gorter RC, Albrecht G, Hoogstraten J, Eijkman MA. Work
place characteristics, work stress and burnout among
Dutch dentists. Eur J Oral Sci 1998;106:999-1005. Crossref
2. Rada RE, Johnson-Leong C. Stress, burnout, anxiety and
depression among dentists. J Am Dent Assoc 2004;135:788-94. Crossref
3. US National Library of Medicine. Depression: what is
burnout? Available from: https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0072470/. Accessed 15 Mar 2017.
4. Maslach C, Jackson SE. Maslach burnout inventory
manual. Mountain View, CA: Consulting Psychologists
Press; 1981.
5. Maslach C. Burned-out. Can J Psychiatr Nurs 1979;20:5-9.
6. Maslach C, Jackson SE. The measurement of experienced
burnout. J Organ Behav 1981;2:99-113. Crossref
7. Maslach C, Jackson SE. Maslach burnout inventory manual.
2nd ed. Mountain View, CA: Consulting Psychologists
Press; 1986.
8. Jin MU, Jeong SH, Kim EK, Choi YH, Song KB. Burnout
and its related factors in Korean dentists. Int Dent J
2015;65:22-31. Crossref
9. Gorter RC, Freeman R. Burnout and engagement in
relation with job demands and resources among dental
staff in Northern Ireland. Community Dent Oral Epidemiol
2011;39:87-95. Crossref
10. Denton DA, Newton JT, Bower EJ. Occupational burnout
and work engagement: a national survey of dentists in the
United Kingdom. Br Dent J 2008;205:E13;discussion 382-3.
11. Siu C, Yuen SK, Cheung A. Burnout among public doctors
in Hong Kong: cross-sectional survey. Hong Kong Med J
2012;18:186-92.
12. Doolittle BR, Windish DM. Correlation of burnout
syndrome with specific coping strategies, behaviors, and
spiritual attitudes among interns at Yale University, New
Haven, USA. J Educ Eval Health Prof 2015;12:41. Crossref
13. Jin WM, Zhang Y, Wang XP. Job burnout and organizational
justice among medical interns in Shanghai, People’s
Republic of China. Adv Med Educ Pract 2015;6:539-44.
14. Portero de la Cruz S, Vaquero Abellán M. Professional
burnout, stress and job satisfaction of nursing staff at a
university hospital. Rev Lat Am Enfermagem 2015;23:543-52. Crossref
15. Singh C, Cross W, Jackson D. Staff burnout—a comparative
study of metropolitan and rural mental health nurses
within Australia. Issues Ment Health Nurs 2015;36:528-37. Crossref
16. Wong MC, Ng KK, Tang AK, Tang GC, Lam VN.
Occupational stress among dental practitioners in Hong
Kong. Hong Kong Dent Assoc Millennium Rep 2001;II:50-5.
17. The Dental Council of Hong Kong. List of registered
dentists under the General Register. Available from: http://www.dchk.org.hk/en/list/index.htm. Accessed 22 Oct
2015.
18. Cooper CL, Watts J, Kelly M. Job satisfaction, mental health,
and job stressors among general dental practitioners in the
UK. Br Dent J 1987;162:77-81. Crossref
19. Waddington TJ. New stressors for GDPs in the past 10
years. Br Dent J 1997;182:82-3. Crossref
20. Kopec JA, Esdaile JM. Occupational role performance in
persons with back pain. Disabil Rehabil 1998;20:373-9. Crossref
21. Gorter RC, Eijkman MA, Hoogstraten J. Burnout and
health among Dutch dentists. Eur J Oral Sci 2000;108:261-7. Crossref