Hong Kong Med J 2018 Jun;24(3):277–84 | Epub 29 May 2018
DOI: 10.12809/hkmj177046
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
REVIEW ARTICLE CME
The effects of global warming on allergic diseases
Alson WM Chan, FHKCPaed, FHKAM (Paediatrics)1;
KL Hon, MD, FHKAM (Paediatrics)2; TF Leung, MD, FHKAM
(Paediatrics)2; Marco HK Ho, MD, FHKAM (Paediatrics)3;
Jaime S Rosa Duque, MD, PhD3,4; TH Lee, ScD(Cantab), FRCP(UK)1
1 Allergy Centre, Hong Kong Sanatorium
& Hospital, Happy Valley, Hong Kong
2 Department of Paediatrics, The Chinese
University of Hong Kong, Shatin, Hong Kong
3 Department of Paediatrics and
Adolescent Medicine, The University of Hong Kong, Pokfulam, Hong Kong
4 Division of Rheumatology and Clinical
Immunology, Department of Medicine, Queen Mary Hospital, The University of
Hong Kong, Pokfulam, Hong Kong
Corresponding author: Dr Alson WM Chan (awmc@hku.hk)
 Full
paper in PDF
Full
paper in PDF
Abstract
Global warming is a public health emergency.
Substantial scientific evidence indicates an unequivocal rising trend in
global surface temperature that has caused higher atmospheric levels of
moisture retention leading to more frequent extreme weather conditions,
shrinking ice volume, and gradually rising sea levels. The concomitant
rise in the prevalence of allergic diseases is closely related to these
environmental changes because warm and moist environments favour the
proliferation of common allergens such as pollens, dust mites, molds,
and fungi. Global warming also stresses ecosystems, further accelerating
critical biodiversity loss. Excessive carbon dioxide, together with the
warming of seawater, promotes ocean acidification and oxygen depletion.
This results in a progressive decline of phytoplankton and fish growth
that in turn promotes the formation of larger oceanic dead zones,
disrupting the food chain and biodiversity. Poor environmental
biodiversity and a reduction in the microbiome spectrum are risk factors
for allergic diseases in human populations. While climate change and the
existence of an allergy epidemic are closely linked according to robust
international research, efforts to mitigate these have encountered
strong resistance because of vested economic and political concerns in
different countries. International collaboration to establish legally
binding regulations should be mandatory for forest protection and energy
saving. Lifestyle and behavioural changes should also be advocated at
the individual level by focusing on low carbon living; avoiding food
wastage; and implementing the 4Rs: reduce, reuse, recycle, and replace
principles. These lifestyle measures are entirely consistent with the
current recommendations for allergy prevention. Efforts to mitigate
climate change, preserve biodiversity, and prevent chronic diseases are
interdependent disciplines.
Introduction
Health hazards that are caused by climate changes
are a major public health emergency of the 21st century. The World Health
Organization estimates that these will lead to 250 000 additional deaths
per year by 2030 to 2050.1
There is substantial evidence for a rising trend of
global surface temperature2 3 4 5 6 7 as demonstrated by the progressive elevation in ocean
temperature and sea level,8 9 the continuous shrinking of polar ice caps,10 11 the rapid
breakup of the Antarctic ice shelves, the melting glaciers at an
increasing rate,12 13 14 15 16 and the
diminishing snow cover in the Northern Hemisphere at an accelerating pace.17 18
19 The subsequent higher
atmospheric levels of moisture retention contribute to more frequent
extreme weather conditions including floods, droughts, thunderstorms,
typhoons, and heat waves.20 21 22 23 24 25 26 27 28 29 30 The rise
in the sea level has been considered to be the greatest threat to the
world in the near future.31 32 33 If global
temperatures continue to increase unabated, sea levels around the world
could rise by up to 5 metres in the next century, and may lead to
submersion of low-lying lands and even countries, such as the Solomon’s
Islands, Maldives, Fiji, and Micronesia. Urban metropolises including Hong
Kong are even more vulnerable to global warming due to the high population
density and essential infrastructures. It has been estimated, for example,
that an increase by 1°C in the mean daily temperature above 28.2°C in Hong
Kong has been associated with a 1.8% higher mortality.25 The annual mean temperature has progressively trended
upwards by 0.12°C per decade from 1885 to 2017, with a more rapid increase
of 0.18°C per decade since the 1980s (Fig 1). The record-breaking highest temperature was
documented on 8 August 2015 with a maximum of 37.9°C measured in Happy
Valley.26 More frequent extreme
precipitation events have also occurred since 2000 and the highest hourly
rainfall of 145.5 mm was observed just recently in 2008. In contrast, in
the last century, the highest recorded hourly rainfall was 110 mm only in
1992. A clear rise in the sea level in Victoria Harbour by an additional
30 mm per decade has been documented since the 1950s.25
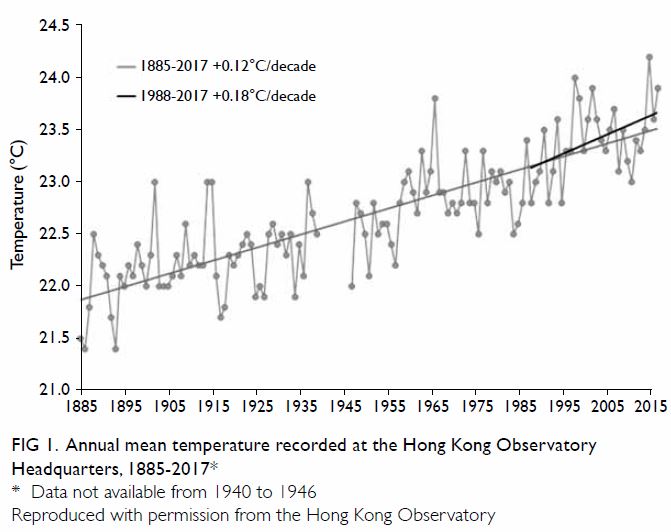
Figure 1. Annual mean temperature recorded at the Hong Kong Observatory Headquarters, 1885-2017
Climate change will continue to accelerate for the
next few decades unless substantial intervening efforts are enforced. It
is projected that by the year 2100, there will be an increase in annual
mean temperature by 3°C to 6°C and there will be significantly greater
annual numbers of very hot days (ie, heat waves, defined as daily maximum
temperature ≥33.0°C) [Fig 2]. Additionally, it is estimated to have a
marked increase from 3 to 12 extremely wet years (ie, annual rainfall
>3168 mm) during the 21st century. The annual mean sea level is
predicted to rise by 0.63 to 1.07 metres, and severe storm surges may
become an annual event whilst these have only occurred once every 50 years
in the past century.27 Nonetheless
these projections are likely to underestimate the actual consequences. For
example, according to the World Meteorological Organization (WMO),
anthropogenic greenhouse gas emissions for 2016 were even higher than
those in 2015, increasing from 400.0 ppm to 403.3 ppm in 12 months.
Although the rate of this increase appears to have slowed, the warming
trend in the climate system will ensure the continued temperature rise
long into the future, leading to progressive temperature rises of up to
5°C to 6°C and with large parts of the Earth potentially uninhabitable in
a foreseeable future.
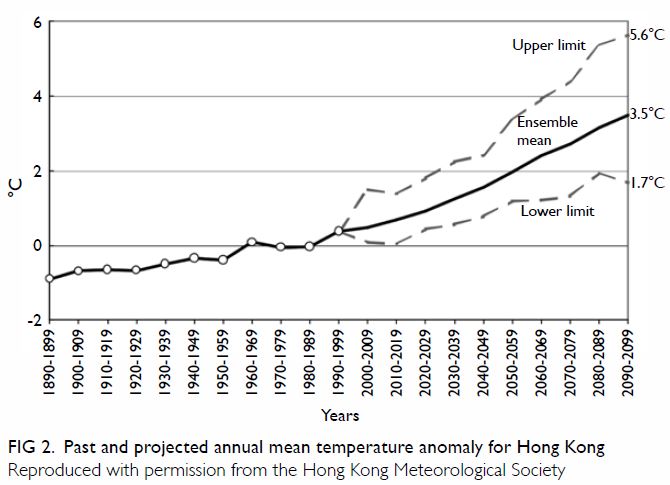
Figure 2. Past and projected annual mean temperature anomaly for Hong Kong
Global warming is a result of human activities.
Fossil fuel consumption and industrial processes account for a majority of
greenhouse gas production. Moreover, in the past 50 years, urbanisation
and intensive agricultural practices have destroyed 50% of global
rainforests. Deforestation, together with excessive fossil fuel combustion
during the process of energy production, result in the imbalance and
progressive accumulation of anthropogenic greenhouse gases. In addition,
carbon dioxide is extremely long-lasting in the atmosphere, with an
average half-life of 30 years. Increased methane emissions, many from
natural gas production and ruminants raised for food, together with other
greenhouse gases such as chlorofluorocarbons used in cooling systems and
nitrous oxide compounds emitted from vehicular transport are even more
powerful but less long-lasting greenhouse gases. These factors contribute
to progressive global warming and extreme weather conditions such as
heatwaves, hurricane storms, floods, forest fires, damage to food crops,
and growing vector-borne diseases, all of which threaten our living
environments and the ecosystem.28
29 30
31
As the global warming situation has continued to
worsen over the past few decades, there has been a concurrent increase in
the prevalence of allergic diseases by up to 300% to 500% in urban areas.
The rate of this increase appears too rapid to be explained entirely by
genetics alone, thereby highlighting the important role of environmental
changes.32
Air pollution and allergic diseases
Epidemiological studies have pointed to a close
correlation between global warming, air pollution, and allergic diseases.33 The process of
industrialisation, increasing vehicle emissions, and a westernised
lifestyle are the major contributors to air pollution. Global warming
contributes to air pollution by increasing the demands for space cooling,
more natural formation of air pollutants (eg, wildfires, soil erosion,
decomposition of organic substances such as plants and animals), and
enhancing the urban heat island effect that causes the formation of
secondary pollutants (such as ozone). Atmospheric pollutants such as
nitric dioxide, ozone, and particulate matter are known to be strongly
associated with allergic respiratory diseases.
Extreme climatic conditions encourage greater
energy utilisation, such as use of heating or air conditioning. This leads
to secondary increases in fossil fuel combustion, worsening of air
pollutants, and accumulation of tropospheric ozone and particulate matter.
Global warming also increases water evaporation and the natural production
of pollutants such as desert sand, sea salt, wildfires, and wood heating,
promoting the growth of pollens, mould spores and the spread of volcanic
ash before they cool down, all of which contribute to the level of
particulates in the air. Indoor air pollution consists mainly of a mixture
of chemical pollutants and allergens, for example, tobacco smoke,
combustion products from heaters and cooking, asbestos, animal allergens,
mycotoxins, fungal allergens, cleaning products, painting, adhesive
solvents, and furniture chemicals. In particular, tobacco smoke contains
at least 3000 compounds, and has five billion particles per cigarette that
significantly adds to air pollution especially within indoor environments.
Diesel particles adhering to pollens have been shown to be more potent in
triggering allergic responses in the airways. Air pollutants affect the
lungs and airways directly by attenuating ciliary activity of epithelial
cells and increasing permeability of the respiratory epithelium. These
effects promote an inflammatory response in the respiratory epithelium and
lung parenchyma.34
Effect of global warming on common allergens
Global warming leads to longer pollination seasons
and more frequent thunderstorms, sandstorms, and other extreme weather
conditions.35 Rising temperatures,
a higher concentration of carbon dioxide in the atmosphere, heavier
rainfalls, and higher humidity induce faster proliferation of pollens,
molds, and fungi. This generates atmospheric biological aerosols that
carry allergens and has caused epidemics of allergic diseases in many
countries.36
Sandstorms or dust storms are meteorological
phenomena that occur more frequently during global warming, at which time
small particles of less than 100 μm can remain airborne for days floating
across hundreds of miles, triggering asthma, pneumonia, allergic
rhinoconjunctivitis, cardiovascular and cerebrovascular diseases.37
Rising temperatures trigger more heavy rainfalls,
frequent storms and the progressive rise in sea levels, causing increased
frequency and duration of floods, subsequently exacerbating the surface
wearing on buildings. These may induce more rapid growth of molds in our
indoor environment. There is a strong and consistent dose-response
relationship between home dampness and respiratory symptoms including
asthma, suggestive of a causal relationship.38
House dust mites and cockroaches prefer warm and humid environments.
Sensitisation to house dust mite is more prevalent in temperate and
tropical regions of the world, and is associated with allergic rhinitis,
allergic conjunctivitis, asthma, and eczema. Nonetheless there are
significant differences in specific house dust mite components that
trigger allergic diseases between different tropical and temperate areas.39 Cockroach allergy is also an
important cofactor for both allergic rhinitis, asthma and eczema, with a
variable pattern of sensitisation within the same climatic zones.40
Effect of global warming on the prevalence of allergic
diseases
Warmer mean temperatures have been shown to be
associated with a higher prevalence of asthma. In a New Zealand study, a
rise in mean temperature of 1°C was associated with an increase in asthma
prevalence by about 1%.41 In an
Italian study that compared two regions with a Mediterranean climate and a
subcontinental climate respectively, a higher mean temperature was also
associated with an increased prevalence of asthmatic attacks.42 In contrast, the International Study of Asthma and
Allergies in Childhood (ISAAC) did not find this same correlation between
mean outdoor temperatures and the prevalence of asthma.43 Nonetheless the ISAAC study was not designed to
specifically investigate the effect of temperature change in different
subregions.
The more frequent thunderstorm and extreme weather
conditions caused by global warming has led to the increased recognition
of thunderstorm asthma. Thunderstorm asthma is a separate entity that
affects many patients without any history of asthma. It usually occurs
during pollen seasons. Epidemics of thunderstorm asthma have been reported
in many countries around the world including the US, United Kingdom,
Australia, and European countries.44
45 46
47 The most alarming event was the
recent epidemic on 21 November 2016 in Melbourne, Australia that resulted
in eight deaths.48 In the time
series analysis for this epidemic reported in the British Medical
Journal, thunderstorm asthma was associated with a 432% increase in
emergency medical attendances for acute respiratory distress symptoms on
that evening, an 82% increase in the incidence of out-of-hospital cardiac
arrest and a 41% increase in prehospital deaths on the same evening of the
storm. It is suggested that grass pollens exploded during the
thunderstorm, producing pollen fragments that could reach the lower
respiratory tract to trigger bronchoconstriction. After the rupture of
those pollens by osmotic force, they released allergenic glycoproteins in
the form of minute respirable particles which were disseminated up to
hundreds of miles.49
Asthma-related hospital admissions have been shown
to be associated with extreme weather conditions. A recent time series
showed an increase in asthma-related hospitalisation during extreme
weather conditions such as the high humidity high temperature weather, the
low humidity low temperature weather, and during periods of high ozone
levels.50 Another recent study
also revealed that the extent of diurnal temperature difference was
positively associated with an increase in hospitalisation due to asthma
exacerbation.51
Out-patient clinic visits for allergic
conjunctivitis were shown to be significantly correlated with higher
levels of nitrous oxide, ozone, and higher temperature in a time series
conducted in Shanghai, China.52
Indoor and outdoor air pollution has been well recognised as a major
environmental risk factor for allergic rhinoconjunctivitis. Associated air
pollutants include tobacco smoke, products of fossil fuel combustion, dust
in Asian region, and phthalates. It is postulated that these air
pollutants may be allergenic, irritant, or a combination of both.53 54 55 56 57
The prevalence of physician-diagnosed allergic
rhinitis has been positively correlated with warmer temperature in studies
along the Pacific rim (odds ratio=1.1, 95% confidence
interval=1.02-1.19).58 Studies using ISAAC data showed some regional
associations in different age-groups and areas, but this observation was
not consistent and has not clearly supported this correlation.59
Increased pollen sensitisation has been correlated
with global warming according to the US National Health and Nutrition
Examination Survey with at least a two-fold rise in the prevalence of
sensitisation to perennial rye grass and ragweed during the two periods
between 1976-1980 and 1988-1994.60
Similar findings were noted in Canada.61
There have been no studies that specifically
focused on a link between urticaria and global warming per se, although a
few anecdotal reports have observed that during high temperatures
associated with global warming patients, tended to wear less clothing,
leading to more light exposure that exacerbated their solar urticaria.62 As for eczema, there is no known correlation between
mean outdoor temperature and its prevalence.
Effect on biodiversity
The scientific evidence is clear: a rich
biodiversity in our living environment is important for human health and
prevention of allergic diseases.63
Nonetheless global warming and population pressures are disrupting
biodiversity in the ecosystem and human living environment.64 For instance, the beginning of the plant growing
season has already advanced by an average of 10 days in Europe over the
last few decades. These changes have altered food chains and created
mismatches within ecosystems where different species have evolved
synchronised interdependence, such as nesting and food availability,
pollinators, and fertilisation. Climate change is also shifting the
habitat ranges of disease-carrying organisms, bringing them into contact
with potential hosts that have not developed any immunity. Freshwater
habitats and wetlands, mangroves, coral reefs, Arctic and alpine
ecosystems, dry and subhumid lands, and cloud forests are particularly
vulnerable to the impacts of climate change. Many species are not equipped
to adapt to the pace and scale of the progressive climate change,
resulting in extinction, both locally and globally. In addition, seawater
warming and ocean acidification due to excessive carbon dioxide lead to a
progressive reduction in the growth of phytoplankton and fish and
overgrowth of bacteria that depletes the oxygen content of water. These
local changes boost the size and extent of oceanic dead zones and
influence the food chain and biodiversity well beyond the Arctic.65
Urban residents have been found to have
significantly more atopy such as asthmatic symptoms, rhinitis, eczema, and
higher exhaled nitric oxide values than those who live in a rural
environment.66 Exposure to the
rich microbial diversity and variety of animals within rural areas plays a
major protective role against the development of asthma and allergic
diseases.67 A number of risk
factors for atopic asthma related to urbanisation have been identified,
including decreased family size and sibling numbers, frequent use of
antibiotics especially during the infantile period, increases in
environmental pollutants and household exposure to indoor allergens,
decreased raw and fresh food consumption, sedentary lifestyle, higher
socio-economic status, and reduction in environmental exposure to
microbial endotoxins.68
Insect migration may be affected by global warming.
In a retrospective review of three different patient databases in Alaska,
there were statistically significant increases in the prevalence of insect
sting reactions accompanying the rise in annual temperatures, suggesting
expansion of the insect habitats and redistribution related to global
warming.69 Invasive insect species
such as destroyer ants and European fire ants are expanding their
influence on humans due to the increase in quantity and quality of
suitable habitats for them related to global warming.70
Food supply and food choice
Global warming leads to more extreme weather
conditions such as heavy rainfalls, drought, frequent storms, floods, and
heat waves. As aforementioned together with the sea warming effect that
also damages the food chain and biodiversity, all of these factors have a
detrimental effect on crop harvest and food production. It has been shown
that an increase in outdoor temperature is associated with a decreasing
trend in the nutrient content and total amount of crop yield per year.71 The fall in food production increases the price of
fresh and raw foods, and encourages consumption of less expensive and
unhealthy food alternatives that contain more artificial colours,
chemicals, and preservatives. Recent research has shown that fresh foods
with natural ingredients contain a richer diversity of microbiome, now
known to be very important for intestinal immune health. On the contrary,
prolonged consumption of preserved or refined foods with a poor diversity
of microbiome is associated with the development of allergic,
inflammatory, cardiovascular, and gastrointestinal diseases.71
Climate change mitigation and allergic disease
prevention
One major challenge for climate change mitigation
is the resistance against countering global warming. In an interview with
CNBC, the US Environmental Protection Agency Administrator and also a
climate change sceptic, Mr Scott Pruitt, stated that he did not believe
carbon dioxide is a cause of global warming. He also described the Paris
Agreement, where representatives from 190 countries agreed to work towards
lowering carbon dioxide emissions, as a ‘bad deal’.72 More than 20 non-profit groups supported him and
contributed more than US$88 million to spread climate science
disinformation via think tanks and advocacy groups to support contrarian
‘science’ intended to create doubt about the prevailing science of
anthropogenic climate change, mostly from fossil fuel interest groups,
following the example of the Big Tobacco’s efforts to derail anti-tobacco
legislation.
Despite this, a large body of scientific evidence
shows that fossil fuel burning is the main cause of climate change. The
use of renewable energy such as solar, wind, ocean, biomass, geothermal
resources for electricity and heat generation to replace conventional
fossil fuel combustion is an important strategy. Reforestation,
afforestation, and avoidance of desertification require multinational and
well-coordinated efforts. For example, China is shifting from fossil fuel
to renewable energy with related investments rising from US$3 billion in
2005 to US$127 billion in 2017, more than the US and EU combined.73 Another example is India’s Forest Rights Act that
aims to strike a balance between agriculture, urbanisation, and forest
protection via legal reinforcement. This act protects the grassland and
national parks from unauthorised agricultural activities and ensures
livestock are fed in designated areas, and places a ban via legal measures
on unauthorised deforestation.74
The inter-governmental panel on climate change established by the United
Nations Environment Programme and the WMO is currently the international
scientific collaborative network focusing on a multinational approach to
climate change mitigation.
Efficient energy use is critical to reduce the
energy consumption. New techniques in home insulation are available that
can help reduce space heating and cooling requirements while maintaining a
comfortable indoor temperature without additional energy consumption.
Lighting using light-emitting diodes or compact fluorescent lights consume
less than a quarter of the energy and are much longer-lasting than
traditional incandescent light bulbs. In addition, the use of skylights
reduces the energy required to attain the same level of illumination and
they are now more commonly incorporated in architectural designs.
Low carbon living is a lifestyle that emits less
carbon dioxide using the 4Rs of environmental protection principles:
reduce, reuse, recycle, and replace. It is becoming an increasingly
important refrain that is being heard more often. Below are some practical
examples: concerning food selection, choose more vegetables and less meat,
more organic and fresh foods rather than processed foods, local production
rather than imported foods, purchase and prepare the amount of food
according to actual need in order to avoid wastage or leftovers, or avoid
accumulation of too much food that cannot be consumed before the expiry
date; bring along reusable storage bags, and avoid restaurants that using
disposable cutlery and crockery such as wooden chopsticks, plastic plates
and plastic bowls; donate excessive food items to food banks before their
expiry; use less oil during cooking (eg, avoid deep frying); send food
waste and packaging for recycling as much as possible; concerning
transportation, use more public transport more often than privately owned
cars; choose less polluting transportation such as Mass Transit Railway,
trams or light buses that use liquefied petroleum gas; walk or cycle if
the destination is nearby, and is healthy and environmentally friendly;
avoid leaving a car engine idling without switching it off; choose an
airline involved in ‘carbon neutral’ programmes when travelling abroad;
concerning energy efficiency: choose grade 1 electrical appliances under
the government’s Energy Efficiency Labelling Scheme; turn off computer
screens, laptops and television completely rather than using the standby
mode; use air conditioners only when the temperature is higher than 26°C,
and set the temperature to about 25.5°C if they are in use.75
Lifestyle and behavioural changes remain the most
important strategies at an individual level. Educational and incentive
programmes should be provided for public stakeholders for environmental
protection. As the prevalence of allergic diseases is correlated with
global warming, a better mitigation of important climatic changes will
help to alleviate the progressive increasing trend of allergic disease
development.
Conclusion
Global warming is caused by human activities. A
paradigm shift should take place to enable everyone to live a healthy and
environmentally friendly lifestyle. Allergy prevention and biodiversity
preservation should not be practised at an individual level only, as it is
a true global health emergency. Strategies must continue to be planned and
coordinated at an international level. Measures to mitigate global
warming, preserve biodiversity, and prevent allergic diseases are
interdependent disciplines that will need to continue to be a major
advocacy and research focus in the next century and beyond.
Declaration
As an editor of this journal, KL Hon was not
involved in the peer review process of this article. All other authors
have no conflicts of interest to disclose. All authors had full access to
the data, contributed to the study, approved the final version for
publication, and take responsibility for its accuracy and integrity.
References
1. World Health Organization. Climate
change and health. Available from:
http://www.who.int/mediacentre/factsheets/fs266/en/. Accessed 27 Sep 2017.
2. Hansen J, Ruedy R, Glascoe J, and Sato
M. GISS analysis of surface temperature change. J Geophys Res
1999;104:30997-1022. Crossref
3. Hansen J, Ruedy R, Sato M, et al. A
closer look at United States and global surface temperature change. J
Geophys Res 2001;106:23947-63. Crossref
4. Karl TR, Trenberth KE. Modern global
climate change. Science 2003;302:1719-23. Crossref
5. Ramaswamy V, Schwarzkopf MD, Randel WJ,
Santer BD, Soden BJ, Stenchikov GL. Anthropogenic and natural influences
in the evolution of lower stratospheric cooling. Science 2006;311:1138-41.
Crossref
6. Marcott SA, Shakun JD, Clark PU, Mix AC.
A reconstruction of regional and global temperature for the past 11,300
years. Science 2013;339:1198-201. Crossref
7. Hausfather Z, Cowtan K, Clarke DC,
Jacobs P, Richardson M, Rohde R. Assessing recent warming using
instrumentally homogeneous sea surface temperature records. Sci Adv
2017;3:e1601207. Crossref
8. Levitus S, Antonov JI, Boyer TP,
Locarnini RA, Garcia HE, Mishonov AV. Global ocean heat content 1955-2008
in light of recently revealed instrumentation problems. Geophys Res Lett
2009;36:L07608. Crossref
9. Church JA, White NJ. A 20th century
acceleration in global sea-level rise. Geophys Res Lett 2006;33:L01602. Crossref
10. Alley RB, Brigham-Grette J, Miller GH,
et al. Past Climate Variability and Change in the Arctic and at High
Latitudes. Washington: US Climate Change Science Program; 2009.
11. Kwok R, Rothrock DA. Decline in Arctic
sea ice thickness from submarine and ICESat records: 1958-2008. Geophys
Res Lett 2009;36:L15501. Crossref
12. Jacob T, Wahr J, Pfeffer WT, Swenson
S. Recent contributions of glaciers and ice caps to sea level rise. Nature
2012;482:514-8. Crossref
13. Gardner AS, Moholdt G, Cogley JG, et
al. A reconciled estimate of glacier contributions to sea level rise: 2003
to 2009. Science 2013;340:852-7. Crossref
14. Marshall S. Climate change. Glacier
retreat crosses a line. Science 2014;345:872. Crossref
15. Marzeion B, Cogley JG, Richter K,
Parkes D. Glaciers. Attribution of global glacier mass loss to
anthropogenic and natural causes. Science 2014;345:919-21. Crossref
16. Zemp M, Frey H, Gärtner-Roer I, et al.
Historically unprecedented global glacier decline in the early 21st
century. J Glaciology 2015;61:745-62. Crossref
17. Groisman PY, Karl TR, Knight RW.
Observed impact of snow cover on the heat balance and the rise of
continental spring temperatures. Science 1994;263:198-200. Crossref
18. Frei A, Robinson DA. Northern
Hemisphere snow extent: regional variability 1972-1994. Int J Climatol
1999;19:1535-60. Crossref
19. Kunkel KE, Robinson DA, Champion S,
Yin X, Estilow T, Frankson RM. Trends and extremes in Northern Hemisphere
snow characteristics. Curr Clim Change Rep 2016;2:65-73. Crossref
20. Kunkel KE, Karl TR, Easterling DR, et
al. Probable maximum precipitation and climate change. Geophys Res Lett
2013;40:1402-8. Crossref
21. Kunkel KE, Karl TR, Brooks H, et al.
Monitoring and understanding trends in extreme storms: state of the
knowledge. BAMS 2013;94:499-514. Crossref
22. Meier MF, Dyurgerov MB, Rick UK, et
al. Glaciers dominate eustatic sea-level rise in the 21st century. Science
2007;317:1064-7. Crossref
23. Bamber J, Riva R. The sea level
fingerprint of recent ice mass fluxes. The Cryosphere 2010;4:621-7. Crossref
24. Radić V, Bliss A, Beedlow AC, Hock R,
Miles E, Cogley JG. Regional and global projections of twenty-first
century glacier mass changes in response to climate scenarios from global
climate models. Clim Dyn 2014;42:37-58. Crossref
25. Chan EY, Goggins WB, Kim JJ, Griffiths
SM. A study of intracity variation of temperature-related mortality and
socioeconomic status among the Chinese population in Hong Kong. J
Epidemiol Community Health 2012;66:322-7. Crossref
26. Hong Kong Observatory. Record-breaking
high temperature [press release]. Available from:
http://www.hko.gov.hk/press/SP/pre20150808.htm. Accessed 16 May 2018.
27. Hong Kong Observatory. Hong Kong in a
warming world. Available from:
http://www.hko.gov.hk/climate_change/climate_change_e.pdf. Accessed 16 May
2018.
28. D’Amato G, Holgate ST, Pawankar R, et
al. Meteorological conditions, climate change, new emerging factors, and
asthma and related allergic disorders. A statement of the World Allergy
Organization. World Allergy Organ J 2015;8:25. Crossref
29. Santer BD, Taylor KE, Wigley TM, et
al. A search for human influences on the thermal structure of the
atmosphere. Nature 1996;382:39-46. Crossref
30. Hegerl GC, von Storch H, Hasselmann K,
Santer BD, Cubasch U, Jones PD. Detecting greenhouse-gas-induced climate
change with an optimal fingerprint method. J Climate 1996;9:2281-306. Crossref
31. Santer BD, Wehner MF, Wigley TM, et
al. Contributions of anthropogenic and natural forcing to recent
tropopause height changes. Science 2003;301:479-83. Crossref
32. Pawankar R, Holgate ST, Canonica GW,
Lockey RF, Blaiss MS, editors. WAO White Book on Allergy: Update 2013.
Milwaukee [WI], US: World Allergy Organization; 2013.
33. Fifth Assessment Report of the
Intergovernmental Panel on Climate Change. Climate Change 2013: The
Physical Science Basis; Summary for Policymakers. Intergovernmental Panel
on Climate Change; 2013.
34. Brunekreef B, Holgate ST. Air
pollution and health. Lancet 2002;360:1233-42. Crossref
35. Ariano R, Canonica GW, Passalacqua G.
Possible role of climate changes in variations in pollen seasons and
allergic sensitizations during 27 years. Ann Allergy Asthma Immunol
2010;104:215-22. Crossref
36. Celenza A, Fothergill J, Kupek E, Shaw
RJ. Thunderstorm associated asthma: a detailed analysis of environmental
factors. BMJ 1996;312:604-7. Crossref
37. Meng Z, Lu B. Dust events as a risk
factor for daily hospitalization for respiratory and cardiovascular
diseases in Minqin, China. Atmos Environ 2007;41:7048-58.
38. Mendell MJ, Mirer AG, Cheung K, Tong
M, Douwes J. Respiratory and allergic health effects of dampness, mold,
and dampness-related agents: a review of the epidemiologic evidence.
Environ Health Perspect 2011;119:748-56. Crossref
39. Banerjee S, Resch Y, Chen KW, et al.
Der p 11 is a major allergen for house dust mite-allergic patients
suffering from atopic dermatitis. J Invest Dermatol 2015;135:102-9. Crossref
40. Potter PC, Motala C, Fenemore B, et
al. Sensitisation to three cockroach species in Southern Africa. Curr
Allergy Clin Immunol 2005;18:62-6.
41. Hales S, Lewis S, Slater T, Crane J,
Pearce N. Prevalence of adult asthma symptoms in relation to climate in
New Zealand. Environ Health Perspect 1998;106:607-10. Crossref
42. de Marco R, Poli A, Ferrari M, et al.
The impact of climate and traffic-related NO2 on the prevalence of asthma
and allergic rhinitis in Italy. Clin Exp Allergy 2002;32:1405-12. Crossref
43. Asher MI, Stewart AW, Mallol J, et al.
Which population level environmental factors are associated with asthma,
rhinoconjunctivitis and eczema? Review of the ecological analyses of ISAAC
Phase One. Respir Res 2010;11:8. Crossref
44. Venables KM, Allitt U, Collier CG, et
al. Thunderstorm-related asthma—the epidemic of 24/25 June 1994. Clin Exp
Allergy 1997;27:725-36. Crossref
45. Marks GB, Colquhoun JR, Girgis ST, et
al. Thunderstorm outflows preceding epidemics of asthma during spring and
summer. Thorax 2001;56:468-71. Crossref
46. Girgis ST, Marks GB, Downs SH, Kolbe
A, Car GN, Paton R. Thunderstorm-associated asthma in an inland town in
south-eastern Australia: who is at risk? Eur Respir J 2000;16:3-8. Crossref
47. Losappio L, Heffler E, Contento F,
Cannito C, Rolla G. Thunderstorm-related asthma epidemic owing to Olea
Europaea pollen sensitisation. Allergy 2011;66:1510-1. Crossref
48. Woodhead M. Hospitals overwhelmed with
patients after “thunderstorm asthma” hits Melbourne. BMJ 2016;355:i6391. Crossref
49. Andrew E, Nehme Z, Bernard S, et al.
Stormy weather: a retrospective analysis of demand for emergency medical
services during epidemic thunderstorm asthma. BMJ 2017;359:j5636. Crossref
50. Lam HC, Li AM, Chan EY, Goggins WB
3rd. The short-term association between asthma hospitalisations, ambient
temperature, other meteorological factors and air pollutants in Hong Kong:
a time-series study. Thorax 2016;71:1097-109. Crossref
51. Qiu H, Yu IT, Tse LA, Chan EY, Wong
TW, Tian L. Greater temperature variation within a day associated with
increased emergency hospital admissions for asthma. Sci Total Environ
2015;505:508-13. Crossref
52. Hong J, Zhong T, Li H, et al. Ambient
air pollution, weather changes, and outpatient visits for allergic
conjunctivitis: A retrospective registry study. Sci Rep 2016;6:23858. Crossref
53. Mimura T, Ichinose T, Yamagami S, et
al. Airborne particulate matter (PM2.5) and the prevalence of allergic
conjunctivitis in Japan. Sci Total Environ 2014;487:493-9. Crossref
54. Mimura T, Yamagami S, Fujishima H, et
al. Sensitization to Asian dust and allergic rhinoconjunctivitis. Environ
Res 2014;132:220-5. Crossref
55. Chang CC, Lee IM, Tsai SS, Yang CY.
Correlation of Asian dust storm events with daily clinic visits for
allergic rhinitis in Taipei, Taiwan. J Toxicol Environ Health A
2006;69:229-35. Crossref
56. World Health Organization. Health
aspects of air pollution with particulate matter, ozone and nitrogen
dioxide. 2003. Available from:
http://www.euro.who.int/__data/assets/pdf_file/0005/112199/E79097.pdf.
Accessed 6 Feb 2018.
57. Bekö G, Callesen M, Weschler CJ, et
al. Phthalate exposure through different pathways and allergic
sensitization in preschool children with asthma, allergic
rhinoconjunctivitis and atopic dermatitis. Environ Res 2015;137:432-9. Crossref
58. Williams R. Climate change blamed for
rise in hay fever. Nature 2005;434:1059. Crossref
59. Weiland SK, Hüsing A, Strachan DP,
Rzehak P, Pearce N; ISSAC Phase One Study Group. Climate and the
prevalence of symptoms of asthma, allergic rhinitis, and atopic eczema in
children. Occup Environ Med 2004;61:609-15. Crossref
60. Arbes SJ Jr, Gergen PJ, Elliott L,
Zeldin DC. Prevalences of positive skin test responses to 10 common
allergens in the US population: results from the third national health and
nutrition examination survey. J Allergy Clin Immunol 2005;116:377-83. Crossref
61. Boulet LP, Turcotte H, Laprise C, et
al. Comparative degree and type of sensitization to common indoor and
outdoor allergens in subjects with allergic rhinitis and/or asthma. Clin
Exp Allergy 1997;27:52-9. Crossref
62. Dice JP. Physical urticarial. Immunol
Allergy Clin North Am 2004;24:225-46. Crossref
63. Haahtela T, Holgate S, Pawankar R, et
al. The biodiversity hypothesis and allergic disease: world allergy
organization position statement. World Allergy Organ J 2013;6:3. Crossref
64. Aukema JE, Pricope NG, Husak GJ,
Lopez-Carr D. Biodiversity areas under threat: overlap of climate change
and population pressures on the world’s biodiversity priorities. PLoS One
2017;12:1. Crossref
65. Convention on Biological Diversity.
Global Biodiversity Outlook 4: A Mid-term Assessment of Progress towards
the Implementation of the Strategic Plan for Biodiversity 2011-2020.
Montréal, Canada: Secretariat of the Convention on Biological Diversity;
2014.
66. Robinson CL, Baumann LM, Romero K, et
al. Effect of urbanisation on asthma, allergy and airways inflammation in
a developing country setting. Thorax 2011;66:1051-7. Crossref
67. Huang YJ, Marsland BJ, Bunyavanich S,
et al. The microbiome in allergic disease: current understanding and
future opportunities-2017 PRACTALL document of the American Academy of
Allergy, Asthma & Immunology and the European Academy of Allergy and
Clinical Immunology. J Allergy Clin Immunol 2017;139:1099-110. Crossref
68. Braun-Fahrländer C, Riedler J, Herz U,
et al. Environmental exposure to endotoxin and its relation to asthma in
school-age children. N Engl J Med 2002;347:869-77. Crossref
69. Demain JG, Gessner BD, McLaughlin JB,
Sikes DS, Foote JT. Increasing insect reactions in Alaska: is this related
to changing climate? Allergy Asthma Proc 2009;30:238-43. Crossref
70. Bertelsmeier C, Luque GM, Courchamp F.
Increase in quantity and quality of suitable areas for invasive species as
climate changes. Conserv Biol 2013;27:1458-67. Crossref
71. Lobell DB, Schlenker W, Costa-Roberts
J. Climate trends and global crop production since 1980. Science
2011;333:616-20. Crossref
72. DiChristopher T. EPA chief Scott
Pruitt says carbon dioxide is not a primary contributor to global warming.
CNBC Politics news. Available from:
https://www.cnbc.com/2017/03/09/epa-chief-scott-pruitt.html. Accessed 30
Jan 2018.
73. Frankfurt School-UNEP Centre/BNEF.
Global Trends in Renewable Energy Investment 2018. Frankfurt School of
Finance & Management gGmbH; 2018.
74. Boysen LR, Lucht W, Gerten D, Heck V,
Lenton TM, Schellnhuber HJ. The limits to global-warming mitigation by
terrestrial carbon removal. Earth’s Future 2017;5:463-74. Crossref
75. Pimm SL, Jenkins CN, Abell R, et al.
The biodiversity of species and their rates of extinction, distribution,
and protection. Science 2014;344:1246752. Crossref