Hong Kong Med J 2016 Feb;22(1):11–5 | Epub 29 Sep 2015
DOI: 10.12809/hkmj144483
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
ORIGINAL ARTICLE
Why do Hong Kong patients need total hip arthroplasty? An analysis of 512 hips from 1998 to 2010
Vincent WK Chan, MB, BS;
PK Chan, FHKCOS, FHKAM (Orthopaedic Surgery);
KY Chiu, FHKCOS, FHKAM (Orthopaedic Surgery);
CH Yan, FHKCOS, FHKAM (Orthopaedic Surgery);
FY Ng, FHKCOS, FHKAM (Orthopaedic Surgery)
Department of Orthopaedics and Traumatology, Queen Mary Hospital, The
University of Hong Kong, Pokfulam, Hong Kong
Corresponding author: Dr Vincent WK Chan (loveholika@gmail.com)
 Full
paper in PDF
Full
paper in PDF
Abstract
Introduction: The number of patients undergoing
total hip replacement surgeries has increased as a
result of a rise in the ageing population. This study
reviewed the demographics and disease spectrum
leading to primary total hip replacement in the
Chinese population from 1998 to 2010.
Methods: This case series was conducted in a
university teaching hospital in Hong Kong. Data
from the prospective joint registry of all patients
who underwent primary total hip replacement from
January 1998 to December 2010 were reviewed.
Patients’ age and sex, diagnosis, as well as the Harris
Hip Scores before operation and at the last follow-up
were described.
Results: There were 512 primary total hip
replacements performed on 419 patients (43.4%
males) during the study period. All had clinical
follow-up for at least 2 years. The mean age of the
patients was 57.6 (standard deviation, 16.6) years.
In males, the main aetiology was osteonecrosis
(50.9%), ankylosing spondylitis (19.5%), and post-traumatic
arthritis (8.5%). For females, it was
osteonecrosis (33.0%), primary osteoarthritis
(18.8%), and post-traumatic arthritis (15.8%).
Alcohol-induced (52.5%) and idiopathic (40.7%)
was the most common cause of osteonecrosis
in males and females, respectively. The mean
preoperative Harris Hip Score and that at last follow-up
was 43.9 (standard deviation, 18.3) and 89.7
(standard deviation, 13.0), respectively.
Conclusions: Osteonecrosis was the most
common aetiology leading to total hip replacement
although there were different causes in both sexes
leading to it. The clinical result in terms of Harris
Hip Score was good for all patients who required
total hip replacement.
New knowledge added by this study
- This study updates the disease pattern and epidemiology underlying the need for primary total hip replacement (THR) in our local Hong Kong population. In addition, the different causes leading to osteonecrosis of the hip were analysed.
- The results of this study could have major implications on public health. They reveal that alcohol and its related health hazards remain a major health concern in Hong Kong. Study of the epidemiology of primary THR may enable us to better allocate our health care resources.
Introduction
Arthritis is a common clinical condition and its
prevalence is increasing worldwide.1 2 3 4 More than
20% of the United States population suffer from
arthritis, and it is estimated that one in four may
develop symptomatic hip osteoarthritis in their lifetime.1 5 It is an important clinical problem and a
major burden on the health care system. Total hip
replacement (THR) significantly improves quality of
life and functional disability.6 7 8 The number of THR
surgeries has been increasing all around the world
over the past 10 years.9 10 11 12
Osteoarthritis is the most common indication
for THR in Caucasian populations. According
to the Annual Report 2013 of the National Joint
Registry for England, Wales and Northern Ireland,
osteoarthritis was the most common cause of
primary THR across all age-groups, accounting for
more than 90% of those aged 50 years and above.10
Overall, 79.2% of primary THRs from 1992 to 2011
in the Swedish population were due to primary
osteoarthritis, with a decreasing trend observed in
THR for inflammatory arthritis.11 As the prevalence
of hip osteoarthritis is lower in Asians,13 the disease
pattern for THR would also be expected to differ. A
review of primary total hip arthroplasty (THA) in the
Hong Kong Chinese population from 1972 to 1997
showed that osteonecrosis was the most common
cause, accounting for 45.6% of cases, while primary
osteoarthritis contributed to 10.2% only.14 Singh et al15 found that in Singapore, 42% of THRs from 2004 to
2006 were due to osteonecrosis. There are no other
recent updates, however.
In view of our ageing population and rising
number of primary THRs, study of the epidemiology
in our locality is important to further plan and
budget our health care resources. This study
reviewed the demographics and disease spectrum
leading to primary THR in the Chinese population
from 1998 to 2010, and attempted to identify any
changes since 1997.
Methods
All patients who underwent primary THR at
Queen Mary Hospital (QMH), a university teaching
hospital in Hong Kong, from January 1998 to December 2010
were reviewed. Diagnosis was made according to
clinical, radiological, and intra-operative findings
and entered by the surgeon. Non-Chinese patients
were excluded from further analysis. Patients’ age
and sex, diagnosis, preoperative and latest Harris
Hip Scores16 at follow-up were analysed. All patients
had clinical follow-up for at least 2 years. The causes
of THR were then compared with the data from 1972
to 1997.14 Chi squared test and Student’s t test were
used for statistical analysis.
Results
A total of 512 THR surgeries were performed on
419 Chinese patients at QMH from January 1998
to December 2010. Of the cases, 43.4% were males
and 48.4% were left hips. The mean (± standard
deviation) age at the time of operation was 57.6 ± 16.6
years. The mean Harris Hip Score at the last follow-up increased significantly compared with that preoperatively (89.7 ± 13.0 vs 43.9 ± 18.3; paired t test, P<0.05) [Table 1].
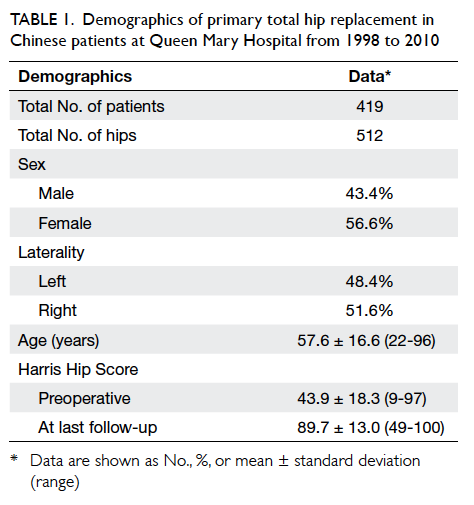
Table 1. Demographics of primary total hip replacement in Chinese patients at Queen Mary Hospital from 1998 to 2010
Osteonecrosis was the most common cause
of primary THR in both males and females in our
study population, accounting for 50.9% and 33.0%,
respectively. The second most common cause
was ankylosing spondylitis in males (19.5%) and
osteoarthritis in females (18.8%). Post-traumatic arthritis was
the third most common cause in both males (8.5%)
and females (15.8%). Rheumatoid arthritis accounted
for 2.5% of primary THRs in males and 9.4% in
females. Dysplasia contributed to 4.1% and 8.0%
of primary THRs in males and females, respectively
(Table 2).
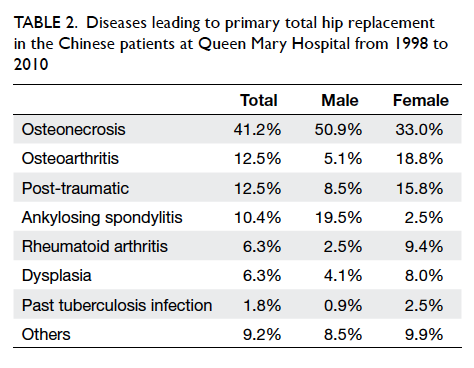
Table 2. Diseases leading to primary total hip replacement in the Chinese patients at Queen Mary Hospital from 1998 to 2010
The underlying causes of osteonecrosis in
females and males were further analysed. The cause
of osteonecrosis was entered by the operating
surgeon based on medical records, as well as clinical,
radiological, and intra-operative findings. The most
common cause of osteonecrosis was alcoholism
in males (52.5%) and idiopathic osteonecrosis in
females (40.7%). Steroid-induced and idiopathic
osteonecrosis was the second and third most
common causes in males, accounting for 26.7% and
15.0%, respectively. In females, steroid-induced and
post-traumatic osteonecrosis was the second and
third most common causes, accounting for 29.7%
and 23.1%, respectively (Table 3).
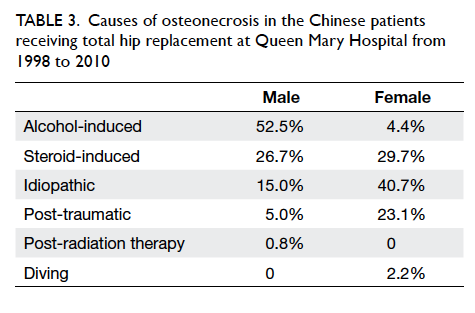
Table 3. Causes of osteonecrosis in the Chinese patients receiving total hip replacement at Queen Mary Hospital from 1998 to 2010
Our data were compared with the results
from a previous study from 1972 to 1997 of primary
THR in the Chinese patients.14 We concluded that
osteonecrosis remains the most common cause
of primary THR in the Chinese population. Other
common causes, such as post-traumatic arthritis, ankylosing
spondylitis and osteoarthritis, showed no statistically
significant changes. The percentage of primary
THR in the Chinese population due to rheumatoid
arthritis, however, has increased significantly from
3.3% to 6.3% (P=0.025; Table 414).
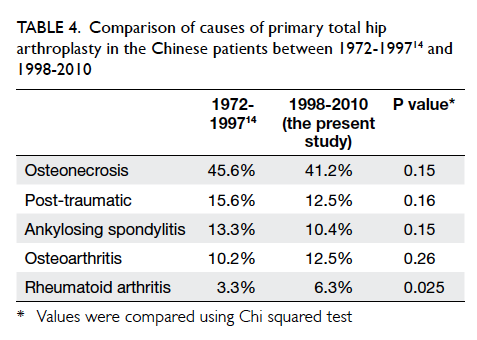
Table 4. Comparison of causes of primary total hip arthroplasty in the Chinese patients between 1972-199714 and 1998-2010
Discussion
Total hip replacement is a well-established surgical
procedure for end-stage arthritis. The number of
THR surgeries is increasing worldwide in parallel
with the rising number of patients with advanced
arthritis. This will place a huge socio-economic
burden on our health care system in the future.
Study of the epidemiology and diseases underlying
the need for THR might help reduce the number
of patients who progress to advanced arthritis, and
in so doing, reduce the burden on our health care
system. In our local community, osteonecrosis was
the most common cause of primary THA from
1972 to 2010.14 Alcoholism was the most common
underlying aetiology of osteonecrosis in men,
accounting for more than 50% of cases. It is evident
that alcoholism remains a major social and health
issue in Hong Kong. The World Health Organization
defines alcoholism as chronic and continual drinking
or periodic consumption of alcohol, characterised
by impaired self-control, frequent intoxication,
and use of alcohol despite adverse consequences.
There is no exact alcohol level that defines
alcoholism. Alcoholism was identified as the cause
of osteonecrosis in our studied patients according to
the clinical context and patient’s social history. The
importance of alcoholism in Hong Kong is further
echoed by a publication by the Department of
Health stating that alcohol consumption per capita
has risen from 2004 to 2010.17 The prevalence of
adult and underage drinking also increased between
2005 and 2010.17 More than 15% of drinkers in Hong
Kong drank beyond the recommended daily limit
in 2010.17 Local and global strategies are needed to
tackle alcoholism and its associated health problems.
Although alcohol is a well-known risk factor
for development of osteonecrosis, the pathogenesis
and dose-response relationship are less established.
Pathological studies in rabbits show that marrow
fat cell hypertrophy and proliferation, thinning of
trabecular, and increased empty osteocyte lacunae
are observed in alcohol-induced osteonecrosis.18
Previous studies proposed that the alcohol exposure
threshold for osteonecrosis in humans is 150 L
of 100% ethanol, consumed at a rate of 400 mL of
absolute ethanol weekly.19 20 More studies, however, are needed to understand the dose and duration
effect of alcohol-induced osteonecrosis.
The Swedish Hip Arthroplasty Register, one of
the earliest registries, is an excellent resource to
study the demographic pattern of joint replacement
in Caucasians. According to their Annual Report
2011, the number of primary THRs steadily
increased from 14 312 in 2007 to 15 945 in 2011.11
Primary osteoarthritis of the hip has been the most
common cause of THA in Sweden for more than 20
years, accounting for 83% in 2011, while idiopathic
osteonecrosis only contributed to 3.2% in 2011.11 On
the contrary, our study showed that osteonecrosis
is the most common cause of THR in the Chinese
population and osteoarthritis accounts for only
12.5%. Such discrepancy is also observed in other
studies in Asian populations. A recent publication
in India found that osteonecrosis was the most
common indication for THR, accounting for 49% of
those performed from 2006 to 2012.21 In Singapore,
42% of THRs were due to osteonecrosis from 2004 to
2006.15 Although the exact underlying mechanism is
unclear, the prevalence of hip osteoarthritis has been
shown to be lower in Orientals than Caucasians.13
The proportion of primary THR performed in
Sweden for inflammatory arthritis decreased over
a period of 5 years, from 2.08% in 2007 to 1.51%
in 2011.11 In the Hong Kong population, however,
the proportion of THR performed for rheumatoid
arthritis increased between 1972-1997 and 1998-2010. We postulate that such discrepancy is due
to our delay in adopting an early strict treatment
strategy for rheumatoid arthritis. It has been shown
by various studies that joint destruction occurs
early in the course of rheumatoid arthritis.22 23 24
Early disease control is essential to prevent joint
destruction and hence, need for joint replacement
surgery. Such a concept had been incorporated in the
European League Against Rheumatism treatment
guideline of 2007.22 Despite this, it is only recently
that the Hong Kong Society of Rheumatology
has modified the local treatment guidelines on
rheumatoid arthritis.25 Future epidemiological study
might be needed to observe any changes in primary
THR requirement for rheumatoid patients.
In this study, the disease leading to THR was
entered by the operating surgeon based on clinical,
radiological, and intra-operative assessments.
Nonetheless, the underlying aetiology is sometimes
difficult to determine in patients with end-stage
arthritis and those with multiple risk factors. This
causes possible information bias, and is a limitation
of this study.
All data within the study period were pooled for
analysis. Hence, any significant changes within the
period from 1998 to 2010 might have been missed.
In addition, data from this study were limited to a
regional hospital in Hong Kong and generalisation
of the results to the present Chinese population
might not be accurate. A total of 15 hospitals were
performing THR within the study period, and QMH
accounted for 15% of surgeries. As a university
teaching hospital, QMH also serves as a tertiary and
quaternary referral centre in Hong Kong, and may
therefore encounter a different disease spectrum
compared with peripheral hospitals in Hong Kong.
We believe a territory or nationwide joint registry,
such as the Swedish Hip Arthroplasty Register or National Joint
Registry (for England, Wales, Northern Ireland),
is needed for more representative results. In view
of the rising number of patients who suffer from
advanced arthritis and hence, the rising number
of joint replacement surgeries, the setting up of a
joint registry is important for further research and
budgeting of our health care resources.
References
1. Centers for Disease Control and Prevention (CDC).
Prevalence of doctor-diagnosed arthritis-attributable
activity limitation—United states, 2003-2005. MMWR
Morb Mortal Wkly Rep 2006;55:1089-92.
2. Centers for Disease Control and Prevention (CDC).
Prevalence of disabilities and associated health conditions
among adults—United States, 1999. MMWR Morb Mortal
Wkly Rep 2001;50:120-5.
3. Stoddard S, Jans L, Ripple J, Kraus L. Chartbook on work
and disability in the United States, 1998: an InfoUse report.
Washington DC: US National Institute on Disability and
Rehabilitation Research; 1998.
4. Hootman JM, Helmick CG. Projections of US prevalence
of arthritis and associated activity limitations. Arthritis
Rheum 2006;54:226-9. Crossref
5. Murphy LB, Helmick CG, Schwartz TA, et al. One in four
people may develop symptomatic hip osteoarthritis in his
or her lifetime. Osteoarthritis Cartilage 2010;18:1372-9. Crossref
6. Ibrahim SA. Racial variations in the utilization of knee and
hip joint replacement: an introduction and review of the
most recent literature. Curr Orthop Pract 2010;21:126-31. Crossref
7. Chang RW, Pellisier JM, Hazen GB. A cost-effectiveness
analysis of total hip arthroplasty for osteoarthritis of the
hip. JAMA 1996;275:858-65. Crossref
8. Emejuaiwe N, Jones AC, Ibrahim SA, Kwoh CK. Disparities
in joint replacement utilization: a quality of care issue. Clin
Exp Rheumatol 2007;25(6 Suppl 47):44-9.
9. Singh JA, Vessely MB, Harmsen WS, et al. A population-based
study of trends in the use of total hip and total knee
arthroplasty, 1969-2008. Mayo Clinic Proc 2010;85:898-904. Crossref
10. National Joint Registry for England, Wales and Northern Ireland 10th Annual Report; 2013.
11. The Swedish Hip Arthroplasty Register Annual Report 2011; 2012.
12. Lai YS, Wei HW, Cheng CK. Incidence of hip replacement
among national health insurance enrollees in Taiwan. J
Orthop Surg Res 2008;3:42. Crossref
13. Lau EM, Symmons DP, Croft P. The epidemiology of hip
osteoarthritis and rheumatoid arthritis in the Orient. Clin
Orthop Relat Res 1996;(323):81-90. Crossref
14. Chiu KY, Ng TP, Poon KC, Ho WY, Yau WP. Primary total
hip replacement in Hong Kong Chinese—a review of 647
hips. Hong Kong J Orthop Surg 1998;2:114-9.
15. Singh G, Krishna L, Das De S. The ten-year pattern of
hip diseases in Singapore. J Orthop Surg (Hong Kong)
2010;18:276-8.
16. Harris WH. Traumatic arthritis of the hip after dislocation
and acetabular fractures: treatment by mold arthroplasty.
An end-result study using a new method of result
evaluation. J Bone Joint Surg Am 1969;51:737-55.
17. Alcohol and health: Hong Kong situation. Hong Kong SAR:
Department of Health. Available from: http://www.dh.gov.hk/english/pub_rec/pub_rec_ar/pdf/ncd_ap2/action_plan_2_alcohol%20and%20health%20HK%20situation_e.pdf. Accessed Sep 2015.
18. Wang Y, Yin L, Li Y, Liu P, Cui Q. Preventive effects of
puerarin on alcohol-induced osteonecrosis. Clin Orthop
Related Res 2008;466:1059-67. Crossref
19. Cruess RL. Osteonecrosis of bone. Current concepts as
to etiology and pathogenesis. Clin Orthop Related Res
1986;(208):30-9.
20. Jones JP Jr. Concepts of etiology and early pathogenesis of
osteonecrosis. Instr Course Lect 1994;43:499-512.
21. Pachore JA, Vaidya SV, Thakkar CJ, Bhalodia HK,
Wakankar HM. ISHKS joint registry: A preliminary report.
Indian J Ortho 2013;47:505-9. Crossref
22. Combe B, Landewe R, Lukas C, et al. EULAR
recommendations for the management of early arthritis:
report of a task force of the European Standing Committee
for International Clinical Studies Including Therapeutics
(ESCISIT). Ann Rheum Dis 2007;66:34-45. Crossref
23. Bakker MF, Jacobs JW, Verstappen SM, Bijlsma JW. Tight
control in the treatment of rheumatoid arthritis: efficacy
and feasibility. Ann Rheum Dis 2007;66 Suppl 3:iii56-60. Crossref
24. Grigor C, Capell H, Stirling A, et al. Effect of a treatment
strategy of tight control for rheumatoid arthritis (the
TICORA study): a single-blind randomised controlled
trial. Lancet 2004;364:263-9. Crossref
25. Mok CC, Tam LS, Chan TH, Lee GK, Li EK; Hong Kong
Society of Rheumatology. Management of Rheumatoid
arthritis: consensus recommendations from the Hong Kong
Society of Rheumatology. Clin Rheumatol 2011;30:303-12. Crossref